
CNS infections — MCQs

A 41-year-old male with a history of Pneumocystis jirovecii pneumonia is found to have multiple ring-enhancing lesions on brain CT. Which of the following is most likely responsible for this patient's abnormal scan?
A 15-year-old boy is brought to the Emergency department by ambulance from school. He started the day with some body aches and joint pain but then had several episodes of vomiting and started complaining of a terrible headache. The school nurse called for emergency services. The boy was born at 39 weeks gestation via spontaneous vaginal delivery. He is up to date on all vaccines and is meeting all developmental milestones. Past medical history is noncontributory. He is a good student and enjoys sports. At the hospital, his blood pressure is 120/80 mm Hg, heart rate is 105/min, respiratory rate is 21/min, and his temperature is 38.9°C (102.0°F). On physical exam, he appears drowsy with neck stiffness and sensitivity to light. Kernig’s sign is positive. An ophthalmic exam is performed followed by a lumbar puncture. An aliquot of cerebrospinal fluid is sent to microbiology. A gram stain shows gram-negative diplococci. A smear is prepared on blood agar and grows round, smooth, convex colonies with clearly defined edges. Which of the following would identify the described pathogen?
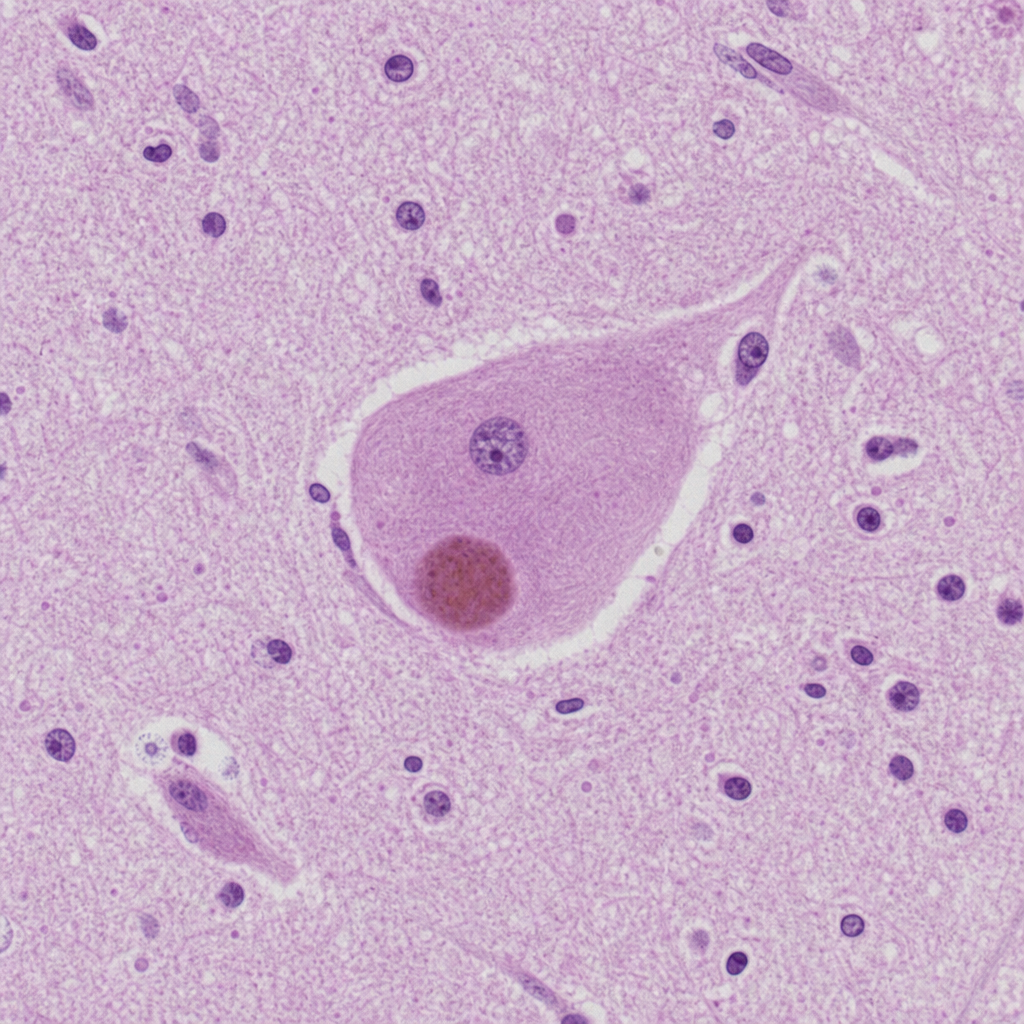
An 81-year-old man is brought to the physician by his daughter after he was found wandering on the street. For the last 3 months, he often has a blank stare for several minutes. He also claims to have seen strangers in the house on several occasions who were not present. He has hypertension and hyperlipidemia, and was diagnosed with Parkinson disease 8 months ago. His current medications include carbidopa-levodopa, hydrochlorothiazide, and atorvastatin. His blood pressure is 150/85 mm Hg. He has short-term memory deficits and appears confused and disheveled. Examination shows bilateral muscle rigidity and resting tremor in his upper extremities. He has a slow gait with short steps. Microscopic examination of the cortex of a patient with the same condition is shown. Which of the following is the most likely diagnosis?
A 65-year-old patient presents with rapidly progressive dementia, myoclonus, and ataxia over 3 months. Laboratory studies, including serum vitamin B12 (cyanocobalamin), thyroxine (T4), and thyroid-stimulating hormone concentrations, are within normal limits. A lumbar puncture is performed. Cerebrospinal fluid (CSF) analysis is most likely to show which of the following?
A 52-year-old man is brought to the emergency department because of headaches, vertigo, and changes to his personality for the past few weeks. He was diagnosed with HIV 14 years ago and was started on antiretroviral therapy at that time. Medical records from one month ago indicate that he followed his medication schedule inconsistently. Since then, he has been regularly taking his antiretroviral medications and trimethoprim-sulfamethoxazole. His vital signs are within normal limits. Neurological examination shows ataxia and apathy. Mini-Mental State Examination score is 15/30. Laboratory studies show: Hemoglobin 12.5 g/dL Leukocyte count 8400/mm3 Segmented neutrophils 80% Eosinophils 1% Lymphocytes 17% Monocytes 2% CD4+ T-lymphocytes 90/μL Platelet count 328,000/mm3 An MRI of the brain with contrast shows a solitary ring-enhancing lesion involving the corpus callosum and measuring 4.5 cm in diameter. A lumbar puncture with subsequent cerebrospinal fluid analysis shows slight pleocytosis, and PCR is positive for Epstein-Barr virus DNA. Which of the following is the most likely diagnosis?
A 13-year-old girl is brought to the physician because of worsening fever, headache, photophobia, and nausea for 2 days. One week ago, she returned from summer camp. She has received all age-appropriate immunizations. Her temperature is 39.1°C (102.3°F). She is oriented to person, place, and time. Physical examination shows a maculopapular rash. There is rigidity of the neck; forced flexion of the neck results in involuntary flexion of the knees and hips. Cerebrospinal fluid studies show: Opening pressure 120 mm H2O Appearance Clear Protein 47 mg/dL Glucose 68 mg/dL White cell count 280/mm3 Segmented neutrophils 15% Lymphocytes 85% Which of the following is the most likely causal organism?
A 67-year-old man presents to the emergency department with confusion. The patient is generally healthy, but his wife noticed him becoming progressively more confused as the day went on. The patient is not currently taking any medications and has no recent falls or trauma. His temperature is 102°F (38.9°C), blood pressure is 126/64 mmHg, pulse is 120/min, respirations are 17/min, and oxygen saturation is 98% on room air. Physical exam is notable for a confused man who cannot participate in a neurological exam secondary to his confusion. No symptoms are elicited with flexion of the neck and jolt accentuation of headache is negative. Initial laboratory values are unremarkable and the patient's chest radiograph and urinalysis are within normal limits. An initial CT scan of the head is unremarkable. Which of the following is the best next step in management?
A 65-year-old man with no significant medical history begins to have memory loss and personality changes. Rapidly, over the next few months his symptoms increase in severity. He experiences a rapid mental deterioration associated with sudden, jerking movements, particularly in response to being startled. He has gait disturbances as well. Eventually, he lapses into a coma and dies approximately ten months after the onset of symptoms. Which of the following would most likely be seen on autopsy of the brain in this patient?
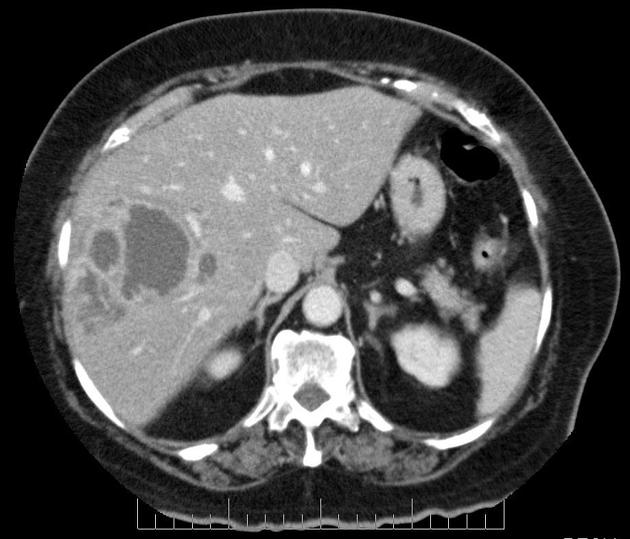
A 40-year-old man presents to the office with complaints of epigastric discomfort for the past 6 months. He adds that the discomfort is not that bothersome as it does not interfere with his daily activities. He does not have any other complaints at the moment. The past medical history is insignificant. He is a non-smoker and does not consume alcohol. He recently came back from a trip to South America where he visited a relative who owned a sheep farm. On physical examination, he has a poorly palpable epigastric non-tender mass with no organomegaly. The hepatitis B and C serology are negative. The liver CT scan and MRI are shown. What is the most likely diagnosis?
A 43-year-old male visits the emergency room around 4 weeks after getting bitten by a bat during a cave diving trip. After cleansing the wound with water, the patient reports that he felt well enough not to seek medical attention immediately following his trip. He does endorse feeling feverish in the past week but a new onset of photophobia and irritability led him to seek help today. What would the post-mortem pathology report show if the patient succumbs to this infection?
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app