
Cerebrovascular diseases — MCQs

A 48-year-old man presents to the ER with a sudden-onset, severe headache. He is vomiting and appears confused. His wife, who accompanied him, says that he has not had any trauma, and that the patient has no relevant family history. He undergoes a non-contrast head CT that shows blood between the arachnoid and pia mater. What is the most likely complication from this condition?
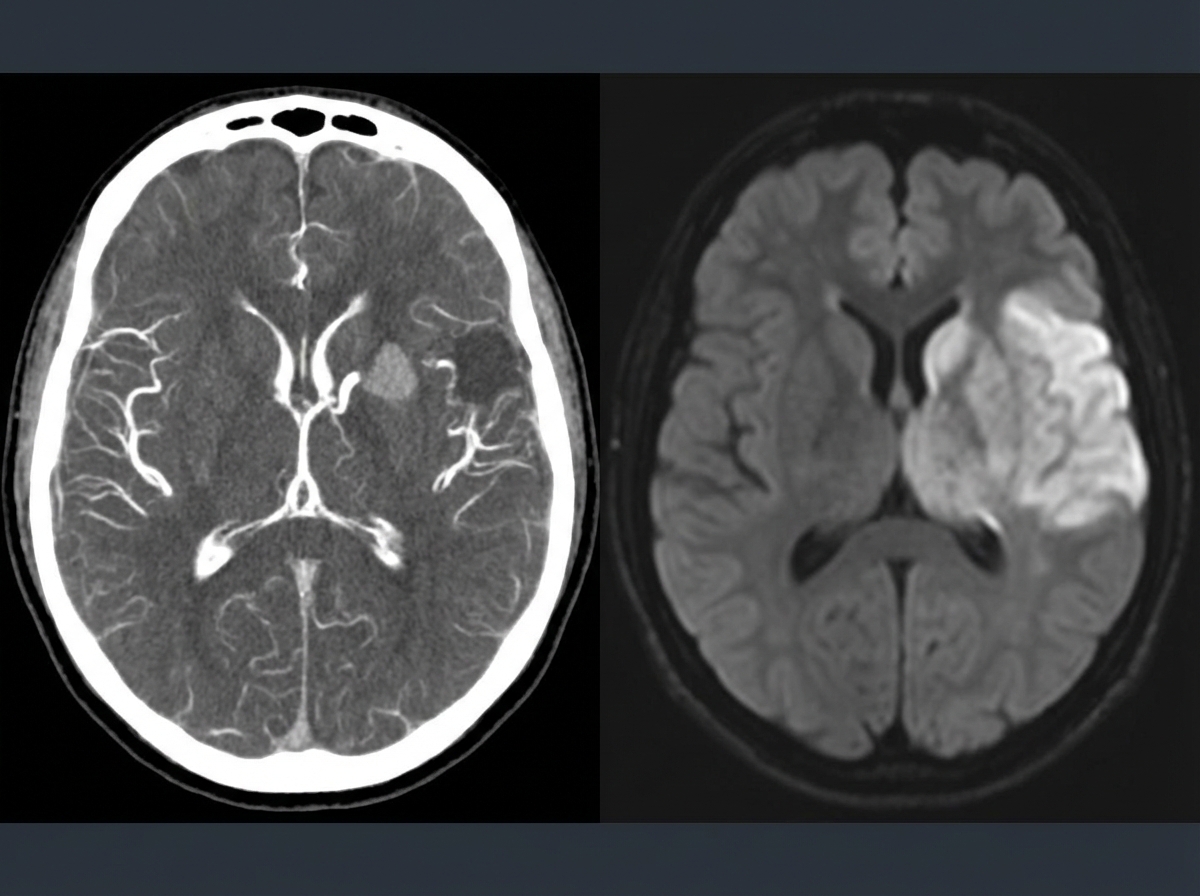
A 69-year-old man is brought in by his wife with acute onset aphasia for the past 5 hours. The patient's wife says that they were sitting having dinner when suddenly he was not able to speak. They delayed coming to the hospital because he had a similar episode 2 months ago which resolved within an hour. His past medical history is significant for hypercholesterolemia, managed with rosuvastatin, and a myocardial infarction (MI) 2 months ago, status post percutaneous transluminal coronary angioplasty complicated by residual angina. His family history is significant for his father who died of MI at age 60. The patient reports a 15-pack-year smoking history but denies any alcohol or recreational drug use. The vital signs include: temperature 37.0℃ (98.6℉), blood pressure 125/85 mm Hg, pulse 96/min, and respiratory rate 19/min. On physical examination, the patient has expressive aphasia. There is a weakness of the right-sided lower facial muscles. The strength in his upper and lower extremities is 4/5 on the right and 5/5 on the left. There is also a decreased sensation on his right side. A noncontrast computed tomography (CT) scan of the head is unremarkable. CT angiography (CTA) and diffusion-weighted magnetic resonance imaging (MRI) of the brain are acquired, and the findings are shown in the exhibit (see image). Which of the following is the best course of treatment in this patient?
A 61-year-old man is brought to the emergency room with slurred speech. According to the patient's wife, they were watching a movie together when he developed a minor headache. He soon developed difficulty speaking in complete sentences, at which point she decided to take him to the emergency room. His past medical history is notable for hypertension and hyperlipidemia. He takes aspirin, lisinopril, rosuvastatin. The patient is a retired lawyer. He has a 25-pack-year smoking history and drinks 4-5 beers per day. His father died of a myocardial infarction, and his mother died of breast cancer. His temperature is 98.6°F (37°C), blood pressure is 143/81 mmHg, pulse is 88/min, and respirations are 21/min. On exam, he can understand everything that is being said to him and is able to repeat statements without difficulty. However, when asked to speak freely, he hesitates with every word and takes 30 seconds to finish a short sentence. This patient most likely has an infarct in which of the following vascular distributions?
A 76-year-old woman with hypertension and coronary artery disease is brought to the emergency department after the sudden onset of right-sided weakness. Her pulse is 83/min and blood pressure is 156/90 mm Hg. Neurological examination shows right-sided facial drooping and complete paralysis of the right upper and lower extremities. Tongue position is normal and she is able to swallow liquids without difficulty. Knee and ankle deep tendon reflexes are exaggerated on the right. Sensation to vibration, position, and light touch is normal bilaterally. She is oriented to person, place, and time, and is able to speak normally. Occlusion of which of the following vessels is the most likely cause of this patient's current symptoms?
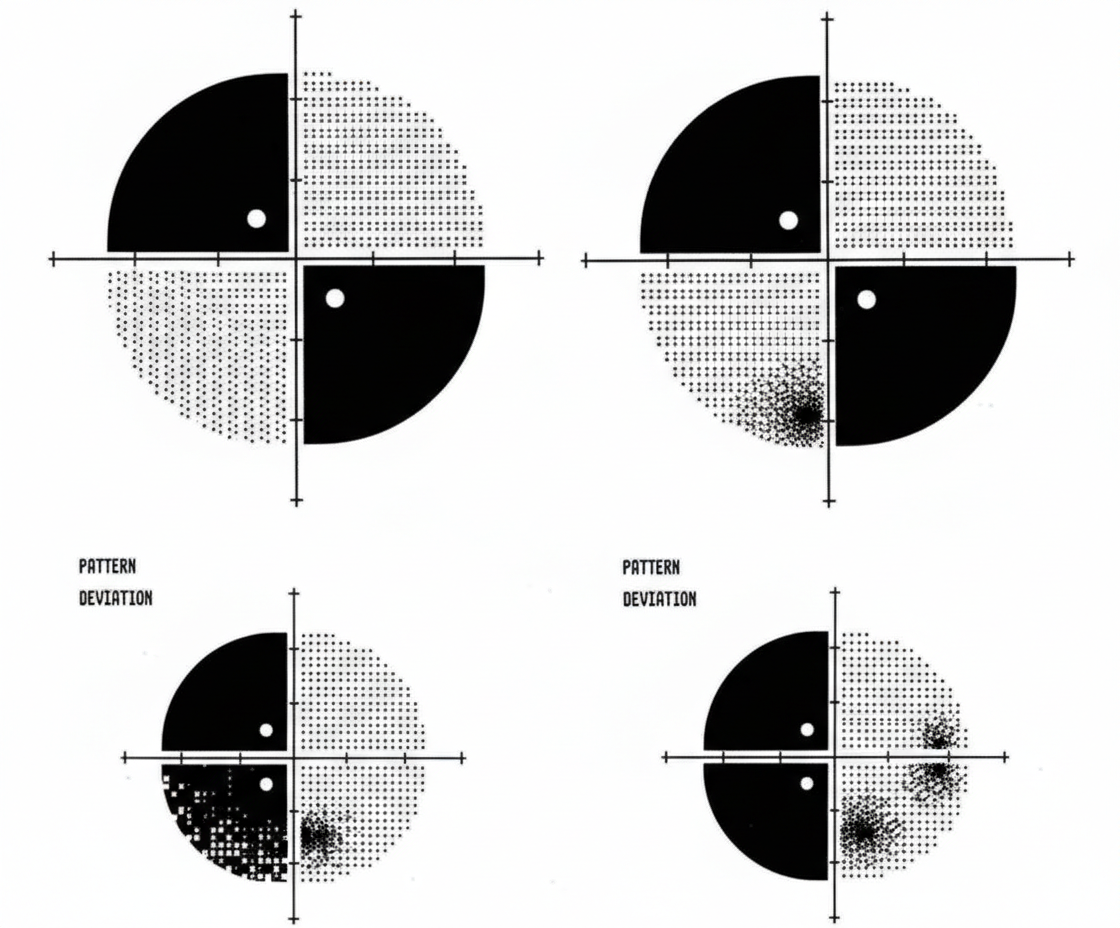
A 62-year-old woman comes to the physician for decreased vision and worsening headaches since this morning. She has hypertension and hypercholesterolemia. Pulse is 119/min and irregular. Current medications include ramipril and atorvastatin. Ocular and funduscopic examination shows no abnormalities. The findings of visual field testing are shown. Which of the following is the most likely cause of this patient's symptoms?
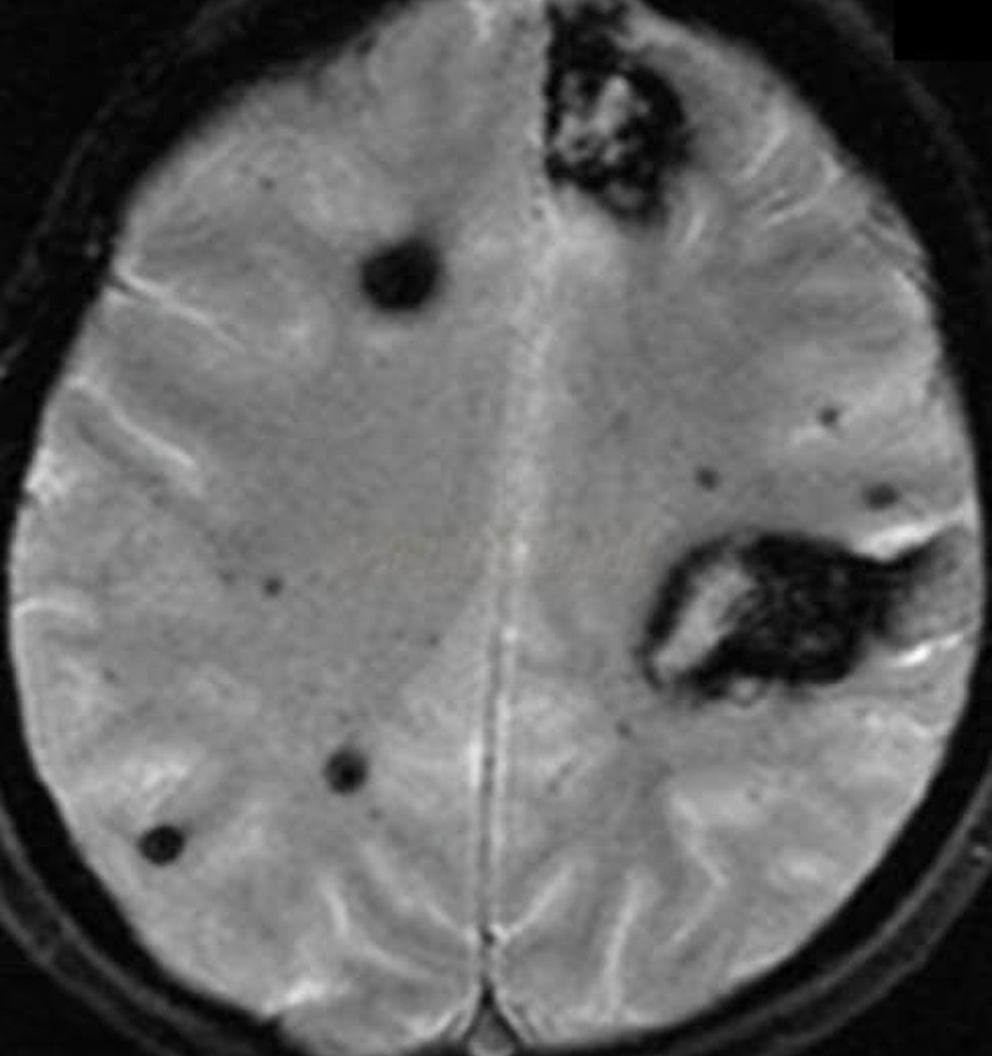
An 88-year-old woman with no significant medical history is brought to the emergency room by her daughter after a fall, where the woman lightly hit her head against a wall. The patient is lucid and complains of a mild headache. The daughter indicates that her mother did not lose consciousness after the fall. On exam, there are no focal neurological deficits, but you decide to perform a CT scan to be sure there is no intracranial bleeding. The CT scan is within normal limits and head MRI is performed (shown). Which of the following conditions has the most similar risk factor to this patient's condition?
A 67-year old woman is brought to the emergency department after she lost consciousness while at home. Her daughter was with her at the time and recalls that her mother was complaining of a diffuse headache and nausea about 2 hours before the incident. The daughter says that her mother has not had any recent falls and was found sitting in a chair when she lost consciousness. She has hypertension. Current medications include amlodipine, a daily multivitamin, and acetaminophen. She has smoked 1/2 pack of cigarettes daily for the past 45 years. Her pulse is 92/min, respirations are 10/min, and blood pressure is 158/100 mm Hg. She is disoriented and unable to follow commands. Examination shows nuchal rigidity. She has flexor posturing to painful stimuli. Fundoscopic examination is notable for bilateral vitreous hemorrhages. Laboratory studies are within normal limits. An emergent non-contrast CT scan of the head is obtained and shows a diffuse hemorrhage at the base of the brain that is largest over the left hemisphere. Which of the following is the most likely cause of this patient's symptoms?
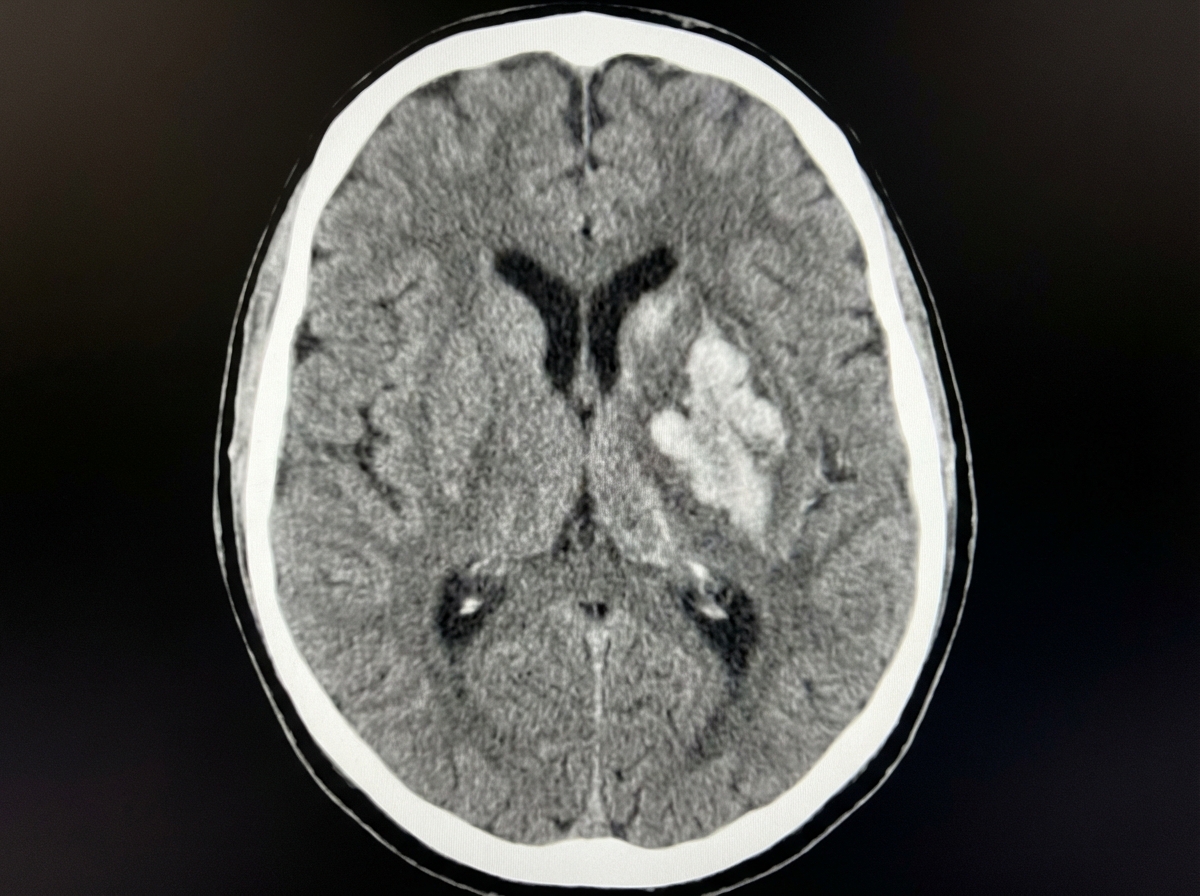
A 68-year-old woman is brought to the emergency department after being found unresponsive in her bedroom in a nursing home facility. Her past medical history is relevant for hypertension, diagnosed 5 years ago, for which she has been prescribed a calcium channel blocker and a thiazide diuretic. Upon admission, she is found with a blood pressure of 200/116 mm Hg, a heart rate of 70/min, a respiratory rate of 15 /min, and a temperature of 36.5°C (97.7°F). Her cardiopulmonary auscultation is unremarkable, except for the identification of a 4th heart sound. Neurological examination reveals the patient is stuporous, with eye-opening response reacting only to pain, no verbal response, and flexion withdrawal to pain. Both pupils are symmetric, with the sluggish pupillary response to light. A noncontrast CT of the head is performed and is shown in the image. Which of the following is the most likely etiology of this patient’s condition?
A 47-year-old man presents as a new patient at an outpatient clinic. He has never seen a physician before, but was motivated by his 40-year-old brother's recent heart attack and seeks to optimize his health. In particular, he read that uncontrolled atherosclerosis can lead to a heart attack. Which molecule is downregulated in response to the advent of atherosclerosis?
A 72-year-old man comes to the physician because of a 6-month history of intermittent dull abdominal pain that radiates to the back. He has smoked one pack of cigarettes daily for 50 years. His blood pressure is 145/80 mm Hg. Abdominal examination shows generalized tenderness and a pulsatile mass in the periumbilical region on deep palpation. Further evaluation of the affected blood vessel is most likely to show which of the following?
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app