
Neoplasia — MCQs

On this page
A 63-year-old man comes to the physician because of increasing generalized fatigue for 3 months. He is having more difficulty with keeping up with his activities of daily living and has lost 2.5 kg (5.5 lb) over the past month. He has hypertension and hyperlipidemia. He does not smoke and drinks two to three beers on weekends. His medications include lisinopril, hydrochlorothiazide, and atorvastatin. His temperature is 37.1°C (98.8°F), pulse is 85/min, respirations are 15/min, and blood pressure is 125/73 mm Hg. Examination shows pale conjunctivae. The remainder of the examination shows no abnormalities. His hematocrit is 27.3%, leukocyte count is 4500/mm3, and platelet count is 102,000/mm3. A peripheral blood smear shows numerous blast cells that stain positive for myeloperoxidase, CD33, and CD34. Which of the following is the most likely diagnosis?
A 62-year-old man comes to the physician because of progressive fatigue and dyspnea on exertion for 3 months. During this time, he has also had increased straining during defecation and a 10-kg (22-lb) weight loss. He has no personal or family history of serious medical illness. Physical examination shows conjunctival pallor. Laboratory studies show microcytic anemia. Test of the stool for occult blood is positive. Colonoscopy shows an exophytic mass in the ascending colon. Pathologic examination of the mass shows a well-differentiated adenocarcinoma. A gain-of-function mutation in which of the following genes is most likely involved in the pathogenesis of this patient's condition?
A 52-year-old man arrives to the clinic for arthritis and leg swelling. The patient reports that the joint pains began 8 months ago. He has tried acetaminophen and ibuprofen without significant improvement. He reports the leg swelling began within the past 2 months and has gotten progressively worse. The patient’s medical history is significant for diabetes. His medications include metformin and aspirin. The patient works as an accountant. He smokes cigars socially. The patient’s temperature is 99°F (37.2°C), blood pressure is 130/78 mmHg, pulse is 70/min, and respirations are 14/min with an oxygen saturation of 98% on room air. Physical examination notes a tan, overweight male with 2+ edema of bilateral lower extremities. Which of the following tumor markers is most likely to be associated with this patient’s condition?
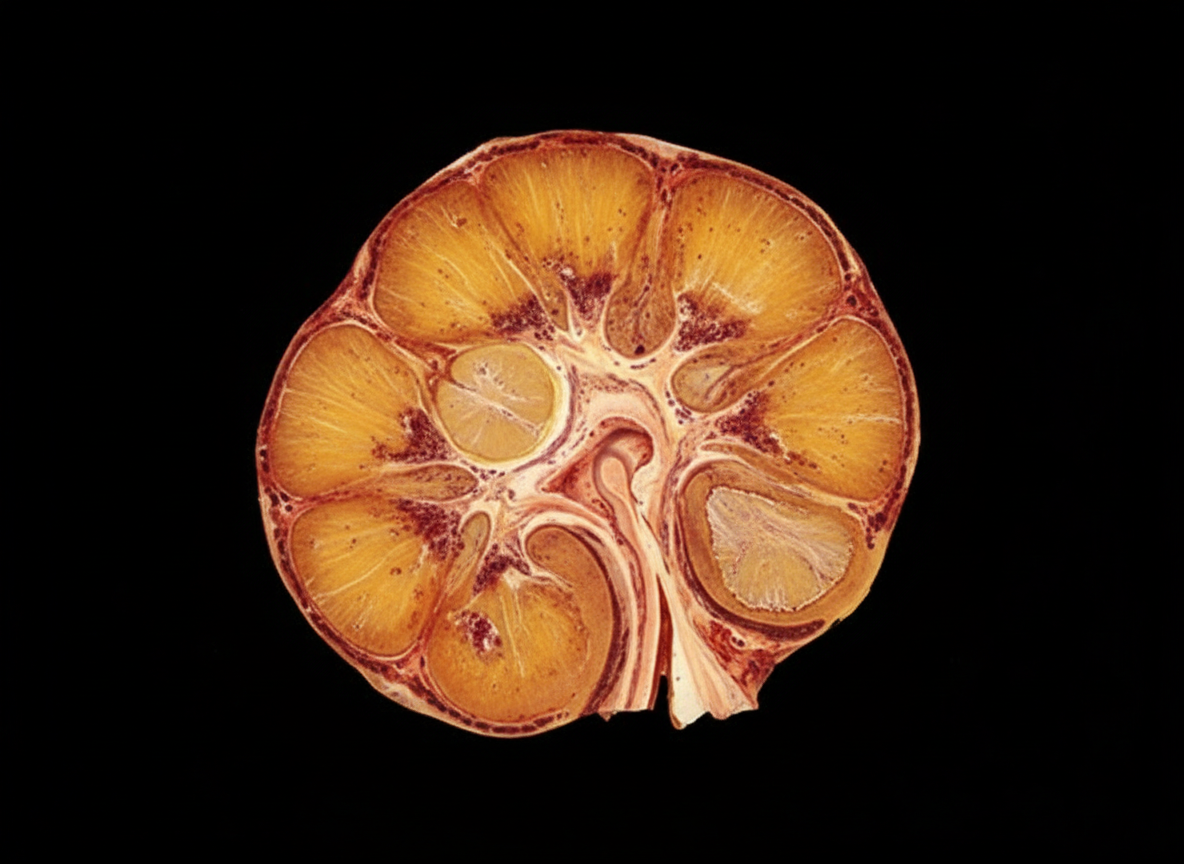
A 75-year-old man comes to the physician because of abdominal pain and nausea over the past 2 weeks and a 1-month history of pain in his knees and hips. He has smoked one pack of cigarettes daily for 30 years. Physical examination shows decreased muscle strength. Laboratory studies show: Hemoglobin 11.0 g/dL Serum Creatinine 1.5 mg/dL Calcium 12.2 mg/dL Parathyroid hormone 8 pg/mL Parathyroid hormone-related peptide elevated Urine Blood 2+ Ultrasonography of his abdomen shows a 6-cm mass in his right kidney. Nephrectomy is performed. A photograph of the resected specimen is shown. The patient's tumor most likely originated from which of the following locations?
A 51-year-old woman comes to the physician because of a persistent cough and a 5-kg (11-lb) weight loss over the past 2 months. Yesterday, she coughed up bloody sputum. She does not smoke. Pulmonary examination shows decreased breath sounds over the right upper lobe. A CT scan of the chest shows a mass in the periphery of the right upper lobe. Histopathologic examination of a specimen obtained on CT-guided biopsy shows glandular cells with papillary components and signet ring cells that stain positive for mucin. An alteration in which of the following genes is most likely to have occurred in this patient?
A 6-year-old boy is brought to a primary care provider by his adoptive parents for evaluation of a 3-month history of jaw swelling. He has a travel history of recent immigration from equatorial Africa where his deceased mother was positive for HIV and died from related complications. On physical exam, extensive lymph node swelling on the left side of his jaw is noted. There is also an ulceration that appears to be infected. Fine needle biopsy of the lymph node yields a diagnosis of Burkitt’s lymphoma by the pathologist. Which of the following is most likely associated with the involvement of lymph nodes around his jaw?
A 74-year-old man comes to the physician for evaluation of a skin lesion on his right arm. The lesion first appeared 3 months ago and has since been slowly enlarging. Physical examination shows a 1.5-centimeter, faintly erythematous, raised lesion with irregular borders on the dorsum of the right forearm. A biopsy specimen is obtained. If present, which of the following histopathological features would be most consistent with carcinoma in situ?
A 45-year-old woman presents to the emergency department after sustaining a gunshot wound to her shoulder. During the course of the physical exam, the physician notes her spleen is palpable 10 cm below the left costal margin. Additionally, radiography of her shoulder showed several 'punched-out' areas of lytic bone. While this was considered an incidental finding at the time, she was referred to her primary care physician for further workup. Subsequent biopsy of the spleen demonstrated that this patient’s splenomegaly was caused by an infiltrative process. Which of the following processes would most likely result in splenomegaly in this patient?
A 67-year-old man presents to the emergency department with increased fatigue. He states that he has been feeling very tired lately but today lost consciousness while walking up the stairs. He reports mild abdominal distension/discomfort, weight loss, a persistent cough, and multiple episodes of waking up drenched in sweat in the middle of the night. The patient does not see a primary care physician but admits to smoking 2 to 3 packs of cigarettes per day and drinking 1 to 3 alcoholic beverages per day. He recently traveled to Taiwan and Nicaragua. His temperature is 99.5°F (37.5°C), blood pressure is 177/98 mmHg, pulse is 100/min, respirations are 17/min, and oxygen saturation is 98% on room air. On physical exam, you note a fatigued appearing elderly man who is well-groomed. Cardiopulmonary exam reveals mild expiratory wheezes. Abdominal exam is notable for a non-pulsatile mass in the left upper quadrant. Laboratory values are ordered as seen below. Hemoglobin: 12 g/dL Hematocrit: 36% Leukocyte count: 105,500/mm^3 Platelet count: 197,000/mm^3 Serum: Na+: 139 mEq/L Cl-: 100 mEq/L K+: 4.3 mEq/L HCO3-: 25 mEq/L BUN: 20 mg/dL Glucose: 92 mg/dL Creatinine: 1.4 mg/dL Ca2+: 10.2 mg/dL Leukocyte alkaline phosphatase score: 25 (range 20 - 100) AST: 12 U/L ALT: 17 U/L Which of the following is the most likely diagnosis?
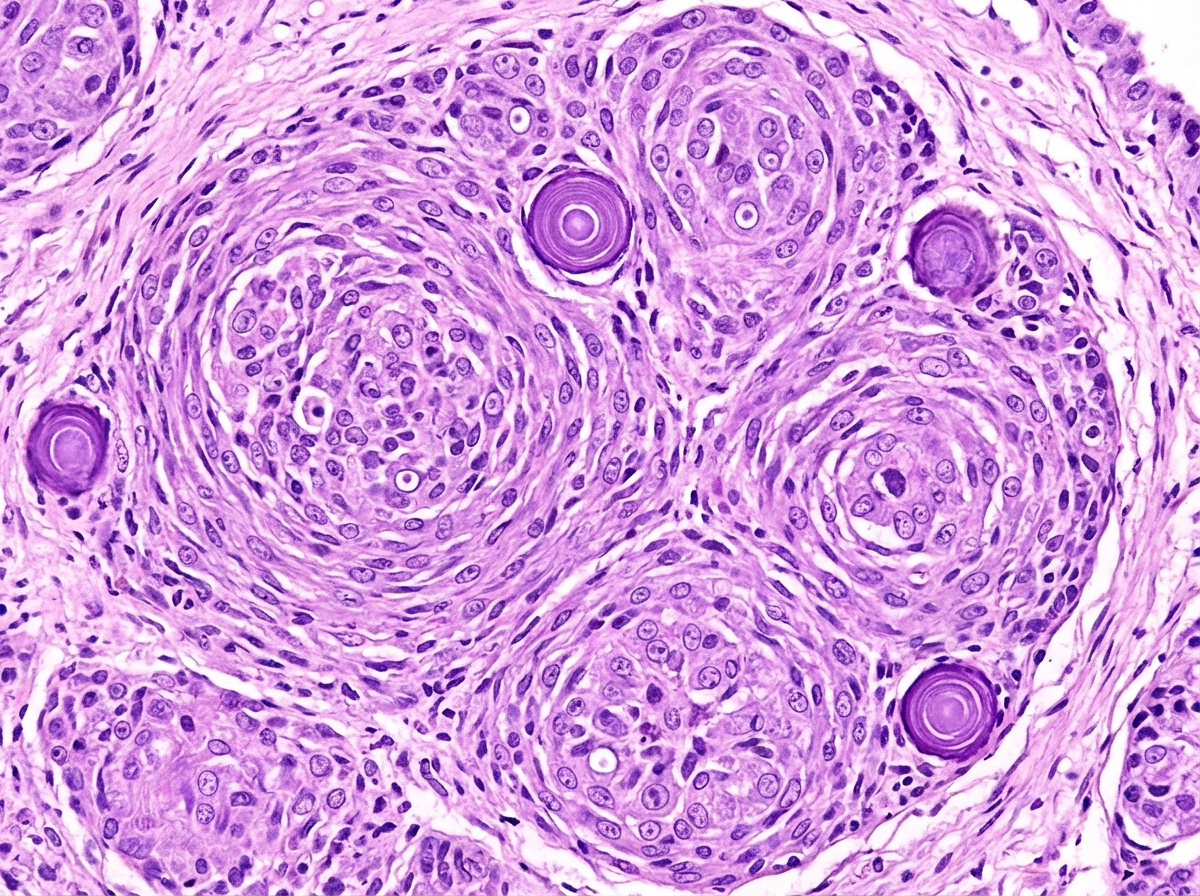
A previously healthy 50-year-old woman is brought to the emergency department 30 minutes after she was observed having a seizure. On arrival, she is conscious and reports that she feels drowsy. An MRI of the brain shows a 4-cm, round, sharply demarcated mass. She undergoes resection of the mass. A photomicrograph of a section of the resected specimen is shown. This patient's mass is most likely derived from which of the following?
Practice by Chapter
Characteristics of benign vs malignant tumors
Practice Questions
Nomenclature of neoplasms
Practice Questions
Carcinogenesis models
Practice Questions
Oncogenes and proto-oncogenes
Practice Questions
Tumor suppressor genes
Practice Questions
DNA repair genes and cancer
Practice Questions
Epigenetic mechanisms in cancer
Practice Questions
Apoptosis and cancer
Practice Questions
Tumor angiogenesis
Practice Questions
Tumor invasion and metastasis
Practice Questions
Carcinogenic agents
Practice Questions
Paraneoplastic syndromes
Practice Questions
Tumor immunology
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app