
Neoplasia — MCQs

On this page
An investigator studying the molecular characteristics of various malignant cell lines collects tissue samples from several families with a known mutation in the TP53 tumor suppressor gene. Immunohistochemical testing performed on one of the cell samples stains positive for desmin. This sample was most likely obtained from which of the following neoplasms?
A 74-year-old retired female teacher is referred to the endocrinology clinic. She is very concerned about a large mass in her neck that has progressively enlarged over the past 2 weeks. She also reports a 15 pound weight loss over the last 3 months. She now has hoarseness and difficulty swallowing her food, giving her a sensation that food gets stuck in her windpipe when she swallows. There is no pain associated with swallowing. Her speech is monotonous. No other gait or language articulation problems are noted. Testing for cranial nerve lesions is unremarkable. On palpation, a large, fixed and non-tender mass in the thyroid is noted. Cervical lymph nodes are palpable bilaterally. The patient is urgently scheduled for an ultrasound-guided fine needle aspiration to guide management. Which of the following is the most likely gene mutation to be found in this mass?
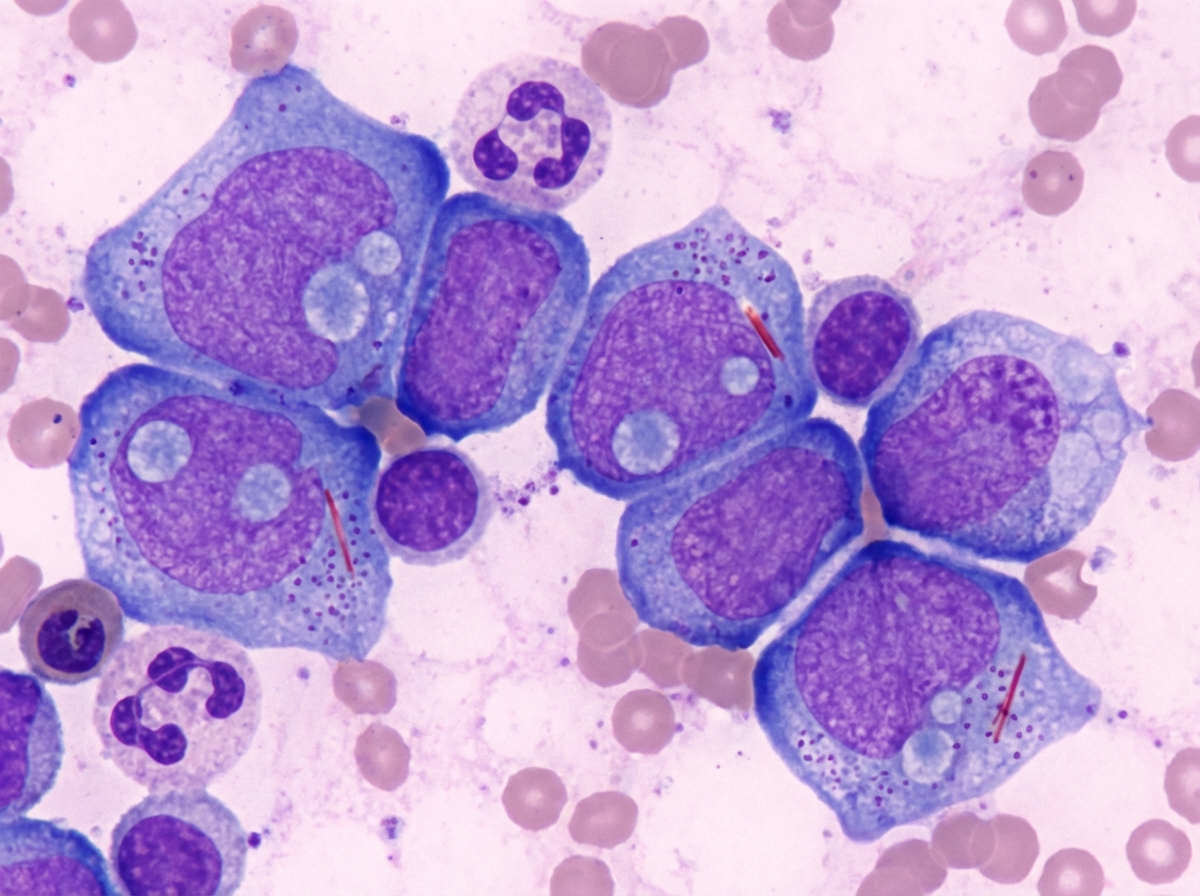
A 59-year-old man comes to the physician because of worsening fatigue and a 1-week history of gingival bleeding. He has also had decreased appetite and a 5-kg (11-lb) weight loss over the past month. He has tried over-the-counter vitamin supplements with no relief of his symptoms. He appears pale. His temperature 37.8° C (100.0°F), pulse is 72/min and blood pressure is 120/70 mm Hg. Physical examination shows numerous petechial lesions over the upper and lower extremities. A bone marrow smear is shown. Which of the following additional findings is most likely in this patient?
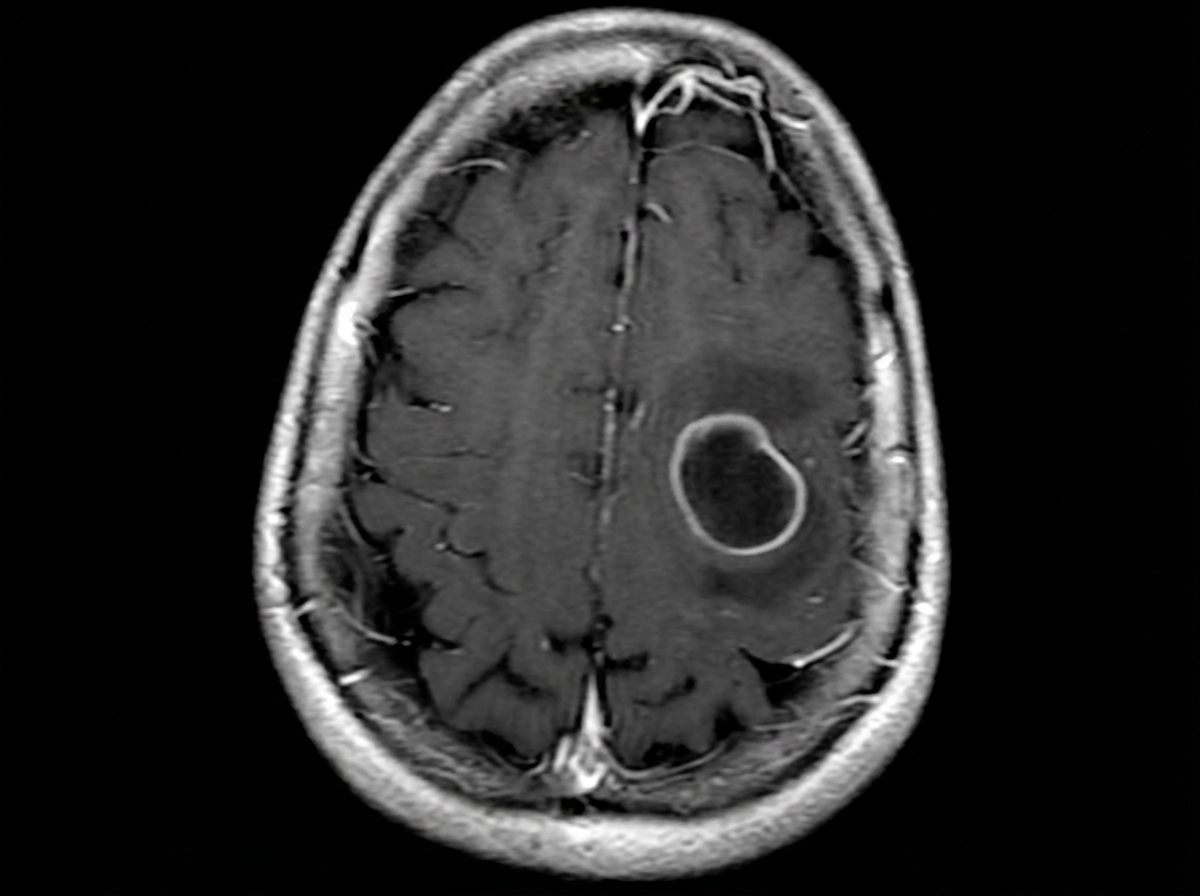
A 61-year-old woman visits the clinic with a complaint of new-onset episodic abnormal body movements. She says her husband noticed it twice in the past week. There were jerky movements for roughly 15 seconds during her last episode. She denies any recent trauma or fever. Her vital signs include: blood pressure 114/74 mm Hg, pulse 81/min, temperature 36.7°C (98.1°F) and respiratory rate 10/min. On physical examination, there is no evidence of focal neurological deficits. A basic metabolic panel is ordered which shows: Sodium 141 mEq/L Potassium 5.1 mEq/L Chloride 101 mEq/L Bicarbonate 24 mEq/L Albumin 4.3 g/dL Urea nitrogen 11 mg/dL Creatinine 1.0 mg/dL Uric Acid 6.8 mg/dL Calcium 8.9 mg/dL Glucose 111 mg/dL A contrast magnetic resonance imaging (MRI) of the head is shown in the provided image. Subsequent stereotactic biopsy of the lesion reveals pseudopalisading necrosis and microvascular proliferation on histopathology. Which of the following cells is the origin of the lesion seen in this patient's MRI?
A 58-year-old man presents with lower back pain that started a couple of weeks ago and is gradually increasing in severity. At present, he rates the intensity of the pain as 6/10. There is no radiation or associated paresthesias. There is no history of trauma. Past medical history is significant for aggressive squamous cell carcinoma of the right lung status post surgical resection followed by adjunct chemotherapy and radiation therapy that was completed 6 months ago. A technetium bone scan reveals metastatic lesions in the lumbar vertebrae at levels L2–L4. The physician explains to the patient that these are likely metastatic lesions from his primary lung cancer. Which of the following best describes the mechanism that most likely led to the development of these metastatic lesions?
A 62-year-old woman comes to the physician for evaluation of a mole on her forearm that has increased in size over the last several months. Physical examination shows a 9-mm skin lesion on the right forearm with irregular borders. An excisional biopsy is performed, and genetic analysis shows a mutation in the gene that encodes B-Raf. Which of the following cellular events most likely predisposed this patient to developing this skin lesion?
A 19-month-old girl is brought by her mother to the local walk-in clinic after noticing a mass protruding from her vagina. The mass had the appearance of "a bunch of grapes". She also says that she has been having a vaginal discharge for the past 6 months. Her family and personal history are not significant for malignancies or inherited disorders. The physical examination is unremarkable except for the presence of soft nodules protruding from the vaginal canal. A tissue sample is obtained for histologic evaluation. Several weeks later the patient returns to the walk-in clinic for a scheduled follow-up visit. The pathology report describes a polypoid mass beneath an epithelial surface with atypical stromal cells positive for polyclonal desmin. What is the most likely diagnosis in this patient?
A 26-year-old nulligravid woman presents to her gynecologist after noticing a lump in her right breast while showering. She states that she first noticed the lump approximately 2 weeks ago, when the mass was slightly tender to touch. Since then, the lump has gotten slightly smaller and is now non-tender. The patient is otherwise healthy. She does not take oral contraceptives. Her last menses was approximately 2 weeks ago. There is no family history of cancer. On exam, the patient's temperature is 98.3°F (36.8°C), blood pressure is 116/84 mmHg, pulse is 65/min, and respirations are 12/min. In her right breast, there is a small 1.5 cm mass that is mobile, well-circumscribed, and firm. Which of the following is most likely on histological examination of the mass?
A 28-year-old patient presents to a medical office for a consultation regarding a mole on her nose that is increasing in size. She also complains of frequent headaches, which she associates with stress on the job. She works as a civil engineer and spends much of her time outside. Her past medical history is positive for bronchial asthma; nevertheless, her vitals are stable. The mole is 8 mm in diameter, has irregular borders, and is brown in color. A biopsy is performed and sent for genetic analysis. A mutation is found. A mutation in which gene is characteristic of this patient’s main diagnosis?
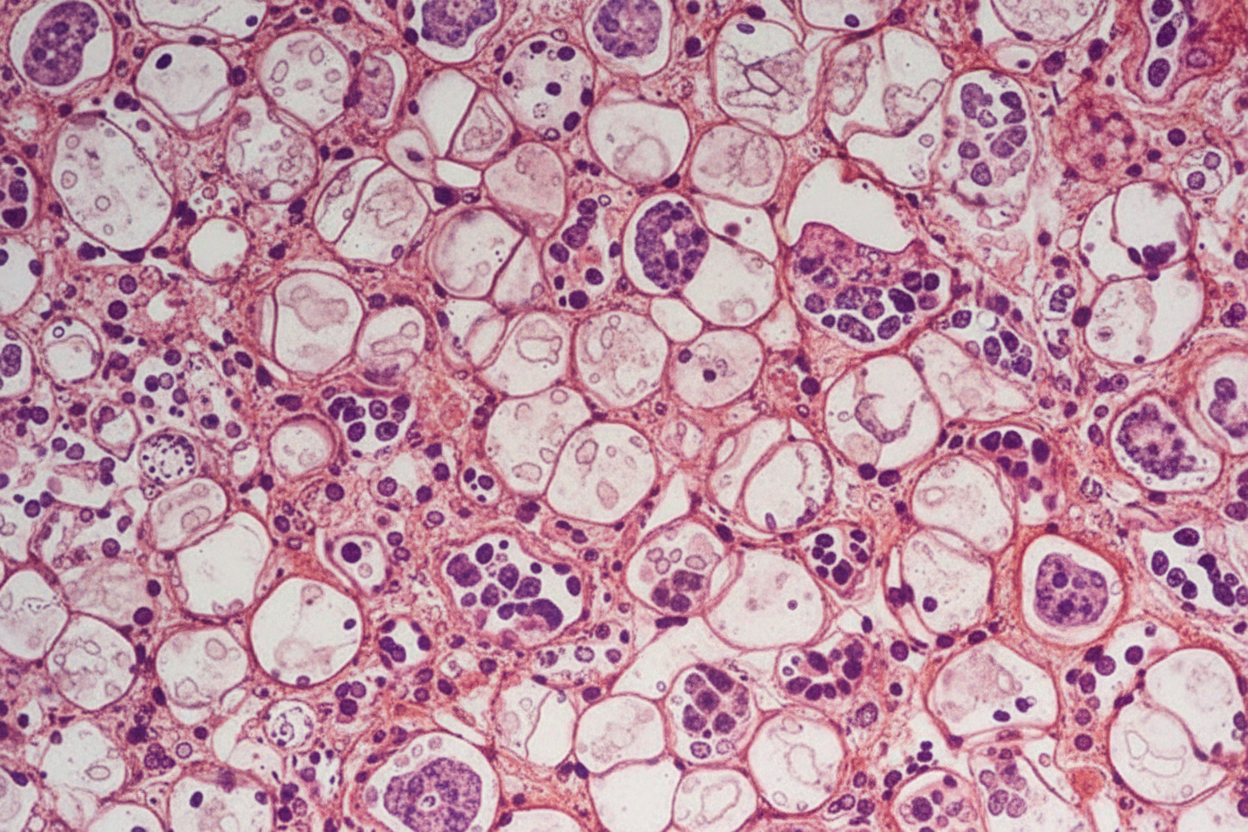
An 82-year-old woman presents to the emergency department because of excruciating right flank pain and fever for the past 2 days. She states that she is having trouble urinating. Her past medical history is unremarkable. A urinalysis is performed and comes back positive for leukocytes and gram-negative bacilli. A contrast computed tomography of the abdomen is performed and reveals a large retroperitoneal mass compressing the right ureter, leading to hydronephrosis of the right kidney. The mass is excised. Histopathologic evaluation of the mass is shown in the image below, and it is determined to be malignant. Which of the following is the most likely diagnosis in this patient?
Practice by Chapter
Characteristics of benign vs malignant tumors
Practice Questions
Nomenclature of neoplasms
Practice Questions
Carcinogenesis models
Practice Questions
Oncogenes and proto-oncogenes
Practice Questions
Tumor suppressor genes
Practice Questions
DNA repair genes and cancer
Practice Questions
Epigenetic mechanisms in cancer
Practice Questions
Apoptosis and cancer
Practice Questions
Tumor angiogenesis
Practice Questions
Tumor invasion and metastasis
Practice Questions
Carcinogenic agents
Practice Questions
Paraneoplastic syndromes
Practice Questions
Tumor immunology
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app