
Neoplasia — MCQs

On this page
A 60-year-old woman comes to the physician because of lower back pain, generalized weakness, and weight loss that has occurred over the past 6 weeks. She also says that her urine has appeared foamy recently. Physical examination shows focal midline tenderness of the lumbar spine and conjunctival pallor. Her temperature is 100.5°F (38°C). A photomicrograph of a bone marrow biopsy specimen is shown. Further evaluation of this patient is most likely to show which of the following findings?
A 72-year-old man presents to the clinic for the evaluation of a lesion on his nose that has been slowly getting larger for the past 2 months. The patient notes no history of trauma, pruritus, or pain, but states that the size of the lesion is making his nose feel uncomfortable. On exam, the nodule is pink with rolled borders. Telangiectasias are also present within the lesion, with central ulceration. What is the characteristic histologic appearance of this lesion?
A 21-year-old male college student is very anxious about having thyroid cancer as he found a lump in his neck a few days ago. He has also had diarrhea and a feeling of warmth on his face for 3 days now. His father and uncle both have been diagnosed with thyroid cancer. The lump is about 1 cm in diameter and is fixed and nontender on palpation. Physical examination is otherwise unremarkable. Ultrasound shows a non-cystic cold nodule that requires fine needle aspiration for diagnosis. Thyroid functions tests are normal, and his calcitonin level is 346 ug/ml. Which of the following genetic mutations would warrant thyroidectomy in this patient?
A 12-year-old boy is brought in by his mother for a routine checkup. The patient’s mother says he is frequently fatigued and looks pale. She also claims that he has recently become “much quieter” than normal and is no longer interested in playing baseball with his friends. The patient’s mother believes it may just be “growing pains.” The patient has no significant medical history. He is the 90th percentile for height and weight and has been meeting all developmental milestones. The patient is afebrile, and his vital signs are within normal limits. Physical examination reveals several small bruises on the patient’s right arm and on both thighs. Laboratory findings are significant for the following: Sodium 140 mEq/L Potassium 4.2 mEq/L Chloride 101 mEq/L Bicarbonate 27 mEq/L BUN 16 mg/dL Creatinine 1.2 mg/dL Glucose (fasting) 111 mg/dL WBC 3,400/mm3 RBC 4.20 x 106/mm3 Hematocrit 22% Hemoglobin 7.1 g/dL Platelet count 109,000/mm3 A peripheral blood smear reveals myeloblasts. Which of the following is the next best step in the management of this patient?
A 62-year-old man comes to the physician because of a 2-month history of an itchy rash and a 7-kg (15-lb) weight loss. Physical examination shows multiple erythematous plaques on the arms, legs, and chest. There are palpable lymph nodes in the axillary and inguinal areas. A biopsy of a skin lesion shows aggregates of neoplastic cells within the epidermis. A peripheral blood smear is most likely to show which of the following findings in this patient?
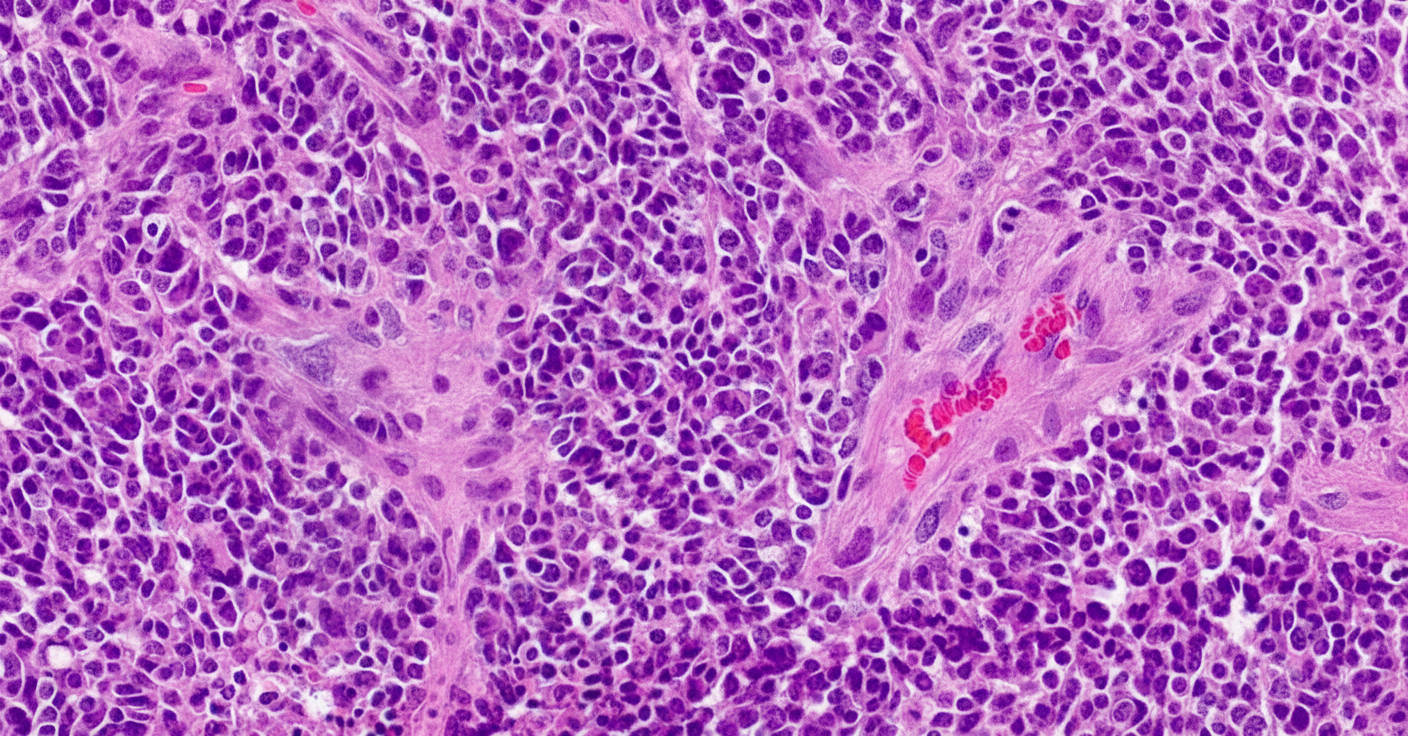
A 10-year-old boy with trisomy 21 arrives for his annual check-up with his pediatrician. His parents explain that over the past week, he has been increasingly withdrawn and lethargic. On examination, lymph nodes appear enlarged around the left side of his neck; otherwise, there are no remarkable findings. The pediatrician orders some routine blood work. These are the results of his complete blood count: WBC 30.4 K/μL RBC 1.6 M/μL Hemoglobin 5.1 g/dL Hematocrit 15% MCV 71 fL MCH 19.5 pg MCHC 28 g/dL Platelets 270 K/μL Differential: Neutrophils 4% Lymphocytes 94% Monocytes 2% Peripheral smear demonstrates evidence of immature cells and the case is referred to hematopathology. On flow cytometry, the cells are found to be CALLA (CD10) negative. Which of the following diseases is most associated with these clinical and cytological findings?
A 55-year-old man comes to the physician because of a 3-day history of decreased urine output, progressively worsening bilateral pedal edema, and fatigue. He has a 4-month history of persistent lower back pain. He has hypercholesterolemia and stable angina pectoris. Current medications include atorvastatin, aspirin, and ibuprofen. His pulse is 80/min, respirations are 16/min, and blood pressure is 150/100 mm Hg. Examination shows periorbital and pedal edema and pallor. There is tenderness of the lumbar spinal vertebrae. Straight leg raise test is negative. The remainder of the examination shows no abnormalities. Laboratory studies show: Hemoglobin 8.9 g/dl Serum Urea nitrogen 20 mg/dl Creatinine 2.4 mg/dl Calcium 11.2 mg/dl Alkaline phosphatase 140 U/L X-ray of the spine shows diffuse osteopenia and multiple lytic lesions. Which of the following is most likely to confirm the diagnosis?
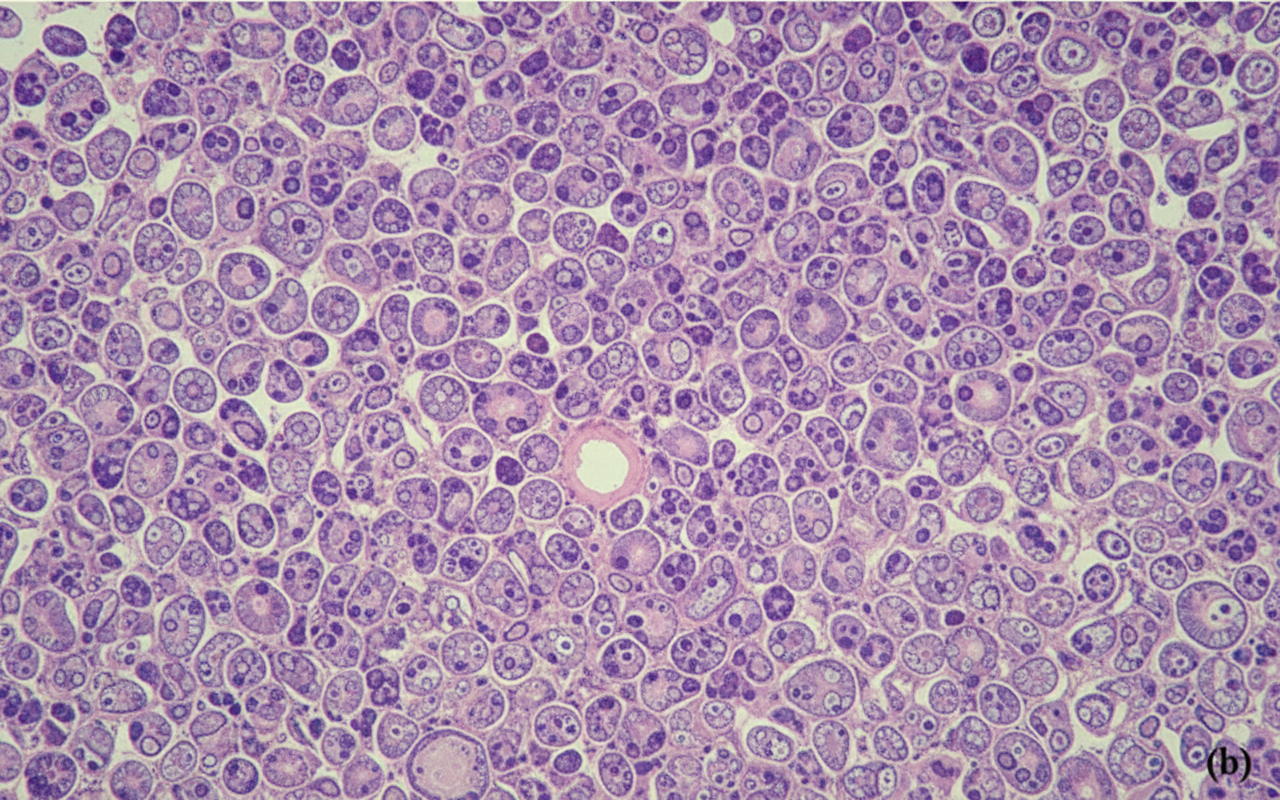
A previously healthy 4-year-old girl is brought to the physician for evaluation of a 3-week history of recurrent vomiting and difficulty walking. Examination shows a broad-based gait and bilateral optic disc swelling. An MRI shows an intracranial tumor. A ventriculoperitoneal shunt is placed, and surgical excision of the tumor is performed. A photomicrograph of a section of the tumor is shown. Which of the following is the most likely diagnosis?
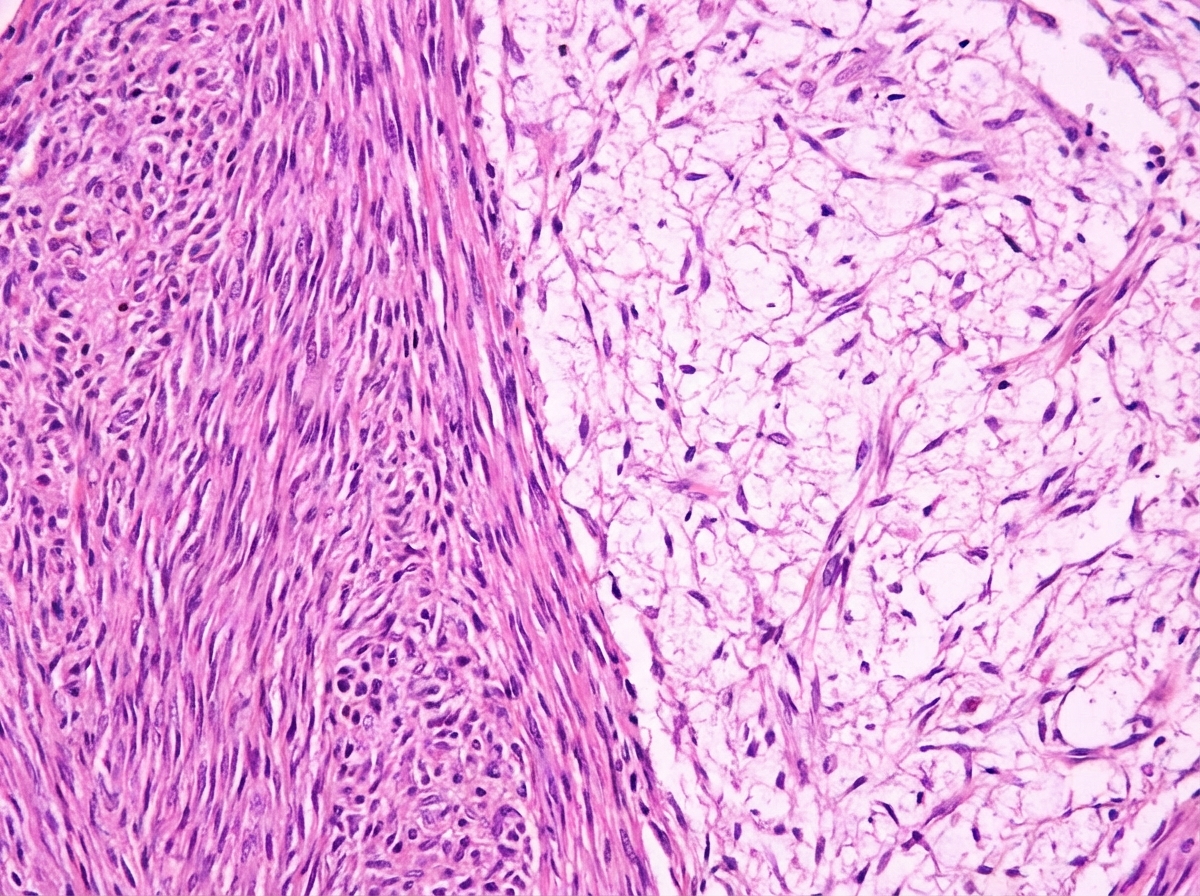
A 35-year-old man, with a history of neurofibromatosis type 2 (NF2) diagnosed 2 years ago, presents with hearing loss in the right ear and tinnitus. Patient says that symptoms have been gradually progressive. He has difficulty hearing speech as well as loud sounds. He also gives a history of occasional headaches and vertigo on and off for 1 month, which is unresponsive to paracetamol. His vitals include: blood pressure 110/78 mm Hg, temperature 36.5°C (97.8°F), pulse 78/min and respiratory rate 11/min. Tuning fork tests reveal the following: Left Right Rinne's test Air conduction > bone conduction Air conduction > bone conduction Weber test Lateralized to left ear Other physical examination findings are within normal limits. An MRI of the head is ordered which is as shown in image 1. A biopsy is done which shows cells staining positive for S100 but negative for glial fibrillary acidic protein (GFAP). The histopathological slide is shown in image 2. What is the most likely diagnosis?
A 68-year-old man comes to the physician because of a 5-month history of undulating, dull pain in his right thigh. Physical examination shows a tender, round mass located above the right knee on the anterior aspect of the thigh. An x-ray of the right thigh shows sunburst pattern of osteolytic bone lesions in combination with sclerotic bone formation and invasion of the surrounding tissue. Despite limb-sparing attempts, the patient has to undergo amputation of the right leg. A photograph of a cross-section of the affected leg is shown. Which of the following is the strongest predisposing factor for this patient's condition?

Practice by Chapter
Characteristics of benign vs malignant tumors
Practice Questions
Nomenclature of neoplasms
Practice Questions
Carcinogenesis models
Practice Questions
Oncogenes and proto-oncogenes
Practice Questions
Tumor suppressor genes
Practice Questions
DNA repair genes and cancer
Practice Questions
Epigenetic mechanisms in cancer
Practice Questions
Apoptosis and cancer
Practice Questions
Tumor angiogenesis
Practice Questions
Tumor invasion and metastasis
Practice Questions
Carcinogenic agents
Practice Questions
Paraneoplastic syndromes
Practice Questions
Tumor immunology
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app