
Neoplasia — MCQs

On this page
A 25-year-old man presents with a mass on his neck. He says that he first noticed the mass a few weeks ago while taking a shower. Since then, the mass has not increased in size. He denies any pain or difficulty in swallowing. Past medical history is unremarkable. Family history is significant for his father who had his thyroid removed when he was around his age but doesn’t know why. Review of systems is significant for occasional episodes of anxiety that include a pounding headache, racing heart, and sweating. His vital signs include: pulse 88/min, blood pressure 133/87 mm Hg, temperature 37.2°C (99.0°F), and respiratory rate 14/min. He is 183 cm (6 ft 2 in) tall with long extremities. On physical examination, the patient appears cachectic. There is a palpable 4 cm x 4 cm nodule present on the left lobe of the thyroid. Which of the following is the most likely thyroid pathology in this patient?
A 65-year-old African-American man presents to your office with dysphagia. He reports that he has found it progressively more difficult to swallow food over the past year. At the time of presentation, he is able to eat only soup. Social history is significant for asbestos exposure, multiple daily drinks of hard alcohol, and a 70 pack-year smoking history. What would you most expect to see on an esophageal biopsy of this patient?
An 8-year-old girl is brought to the clinic by her parents for fever and easy bruising. Her parents report that the child has been bruising easily ever since an upper respiratory infection 3 months ago. For example, a bump into the table resulted in a large bruise on the side of her hip for a week. Three days ago, her mother noticed that the child felt warm and subsequently measured a temperature of 101.8°F (38.8°C) that did not respond to acetaminophen. The patient denies any chills, cough, rhinorrhea, pharyngitis, sick contacts, headache, or urinary symptoms. A physical examination demonstrates a nontender, firm, and rubbery node along her left neck and splenomegaly. Laboratory findings are shown below: Leukocyte count and differential: Leukocyte count: 19,000/mm³ Neutrophils: 39% Bands: 12% Eosinophils: 2% Basophils: 0.5% Lymphocytes: 40% Monocytes: 6.5% Hemoglobin: 9.7 g/dL Platelet count: 100,000/mm³ Mean corpuscular hemoglobin concentration: 30% Mean corpuscular volume: 76 μm³ Reticulocyte count: 0.7% What cytogenetic abnormality would be most likely in this patient?
A 19-year-old man comes to the physician because of a 2-day history of blood-speckled stools and a protruding rectal mass. He has no abdominal pain, altered bowel habits, or fever. His mother has inflammatory bowel disease. His vital signs are within normal limits. Examination shows multiple, small, hyperpigmented maculae on the lips, buccal mucosa, palms, and soles. The abdomen is soft with no organomegaly. Rectal examination shows a 4-cm pedunculated polyp with superficial excoriations on the mucosa. A colonoscopy shows 14 polyps. A biopsy shows hamartomatous mucosal polyps. This patient's diagnosis is most likely?
A 42-year-old woman is seen by her primary care physician for her annual checkup. She has no current concerns and says that she has been healthy over the last year except for a bout of the flu in December. She has no significant past medical history and is not currently taking any medications. She has smoked 1 pack per day since she was 21 and drinks socially with her friends. Her family history is significant for prostate cancer in her dad when he was 51 years of age and ovarian cancer in her paternal aunt when she was 41 years of age. Physical exam reveals a firm, immobile, painless lump in the upper outer quadrant of her left breast as well as 2 smaller nodules in the lower quadrants of her right breast. Biopsy of these lesions shows small, atypical, glandular, duct-like cells with stellate morphology. Which of the following pathways is most likely abnormal in this patient?
A 9-year-old girl is brought to her primary care physician because of a 4-month history of early morning headaches and worsening fatigue. The headaches are often accompanied by nausea and sometimes relieved by vomiting. She stopped going to her ballet lessons 2 weeks ago because she was embarrassed about falling frequently and having increasing difficulty performing the steps. Her temperature is 36.8°C (98.2°F), pulse is 98/min, and blood pressure is 105/65 mm Hg. She has a broad-based gait. While standing with both feet together and raising her arms, closing her eyes does not affect her balance. She is unable to perform rapid, alternating movements with her hands. An MRI of the brain is shown. Which of the following is the most likely diagnosis?

A sexually active 37-year-old man comes to the physician because of a 7-day history of itching in the area of his genitals. He also reports burning on micturition. He has type 2 diabetes mellitus, which is well controlled with oral metformin. Pelvic examination shows tender, atrophic white papules on the glans and prepuce, with erythema of the surrounding skin. The urinary meatus is narrowed and sclerotic. Which of the following is the most appropriate next step in diagnosis?
A 29-year-old man comes to the physician because of a 3-month history of fatigue, weight loss, and multiple painless swellings on his neck and axilla. He reports that his swellings become painful after he drinks alcohol. Physical examination shows nontender cervical and axillary lymphadenopathy. A lymph node biopsy specimen shows giant binucleate cells. Which of the following is the most likely diagnosis?
A 32-year-old Caucasian man presents to the physician because of the swelling and discomfort of the right testis for 3 weeks. There is no history of trauma, fever, or night sweats. He had surgery for an undescended right testis when he was 6 months old. There is no history of liver disease or hypogonadism. He has fathered 2 children. He takes no medications and denies any illicit drug use. The vital signs are within normal limits. Palpation of the scrotum reveals a firm nontender mass that cannot be separated from the right testis. Examination of the left testis shows no abnormalities. There is no supraclavicular or inguinal lymphadenopathy. Gynecomastia is present. The rest of the physical examination is unremarkable. Ultrasound shows an enlarged right testicle with a hypoechoic mass replacing a large portion of the normal architecture. The left testis is normal. The laboratory test results are as follows: HCG Elevated AFP Elevated LDH Normal Which of the following is the most likely diagnosis?
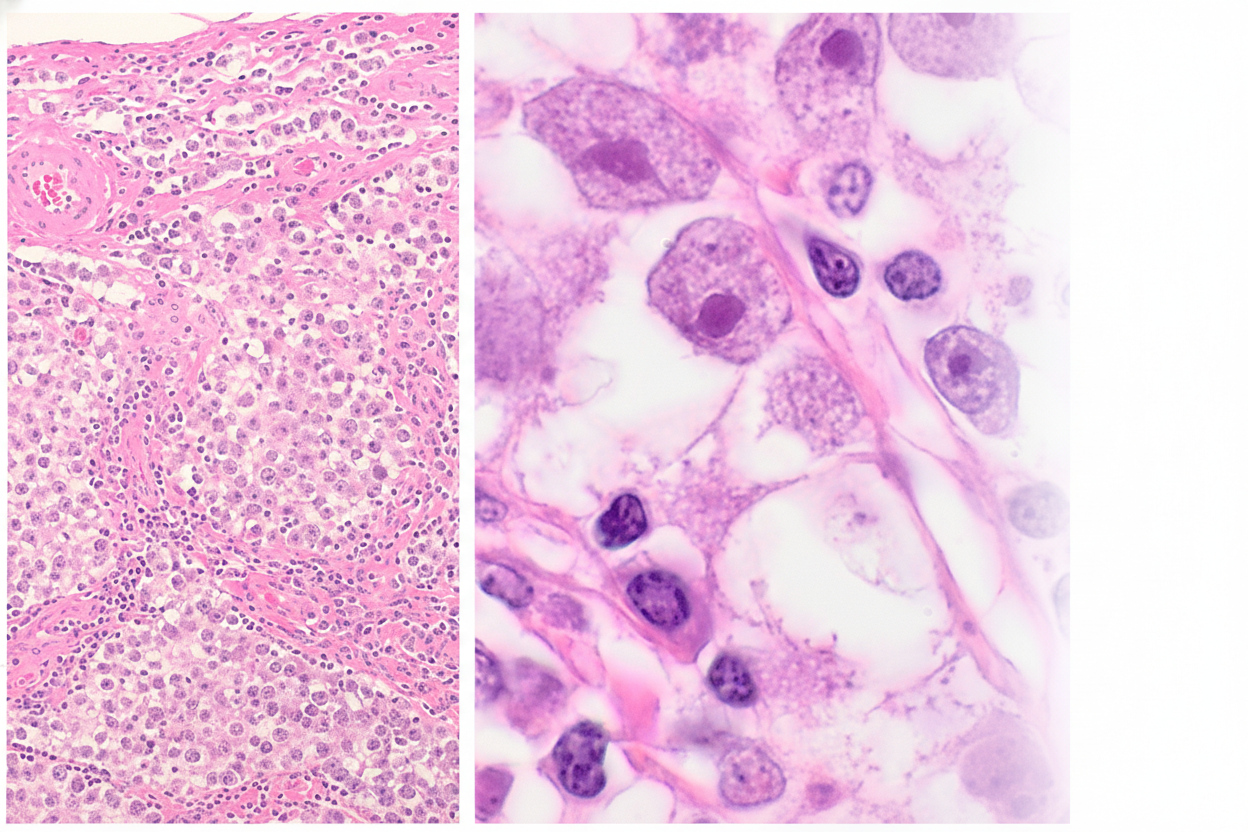
A 22-year-old man comes to the physician for the evaluation of a 2-day history of right testicular pain. At the age of 6 months, he was treated for hypospadias and cryptorchidism. Physical examination shows a rubbery, large right testicle. Orchidectomy is performed. A photomicrograph of a section of the mass is shown. Which of the following additional physical examination findings is most likely in this patient?
Practice by Chapter
Characteristics of benign vs malignant tumors
Practice Questions
Nomenclature of neoplasms
Practice Questions
Carcinogenesis models
Practice Questions
Oncogenes and proto-oncogenes
Practice Questions
Tumor suppressor genes
Practice Questions
DNA repair genes and cancer
Practice Questions
Epigenetic mechanisms in cancer
Practice Questions
Apoptosis and cancer
Practice Questions
Tumor angiogenesis
Practice Questions
Tumor invasion and metastasis
Practice Questions
Carcinogenic agents
Practice Questions
Paraneoplastic syndromes
Practice Questions
Tumor immunology
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app