
Neoplasia — MCQs

On this page
A 40-year-old female comes in with several months of unintentional weight loss, epigastric pain, and a sensation of abdominal pressure. She has diabetes well-controlled on metformin but no other prior medical history. She has not previously had any surgeries. On physical exam, her doctor notices brown velvety areas of pigmentation on her neck. Her doctor also notices an enlarged, left supraclavicular node. Endoscopic findings show a stomach wall that appears to be grossly thickened. Which of the following findings would most likely be seen on biopsy?
A 67-year-old woman presents to a surgeon with a painless, slowly growing ulcer in the periauricular region for the last 2 months. On physical examination, there is an irregular-shaped ulcer, 2 cm x 1 cm in its dimensions, with irregular margins and crusting over the surface. The woman is a fair-skinned individual who loves to go sunbathing. There is no family history of malignancy. After a complete physical examination, the surgeon performs a biopsy of the lesion under local anesthesia and sends the tissue for histopathological examination. The pathologist confirms the diagnosis of squamous cell carcinoma of the skin. When she asks about the cause, the surgeon explains that there are many possible causes, but it is likely that she has developed squamous cell carcinoma on her face due to repeated exposure to ultraviolet rays from the sun, especially ultraviolet B (UVB) rays. If the surgeon’s opinion is correct, which of the following mechanisms is most likely involved in the pathogenesis of the condition?
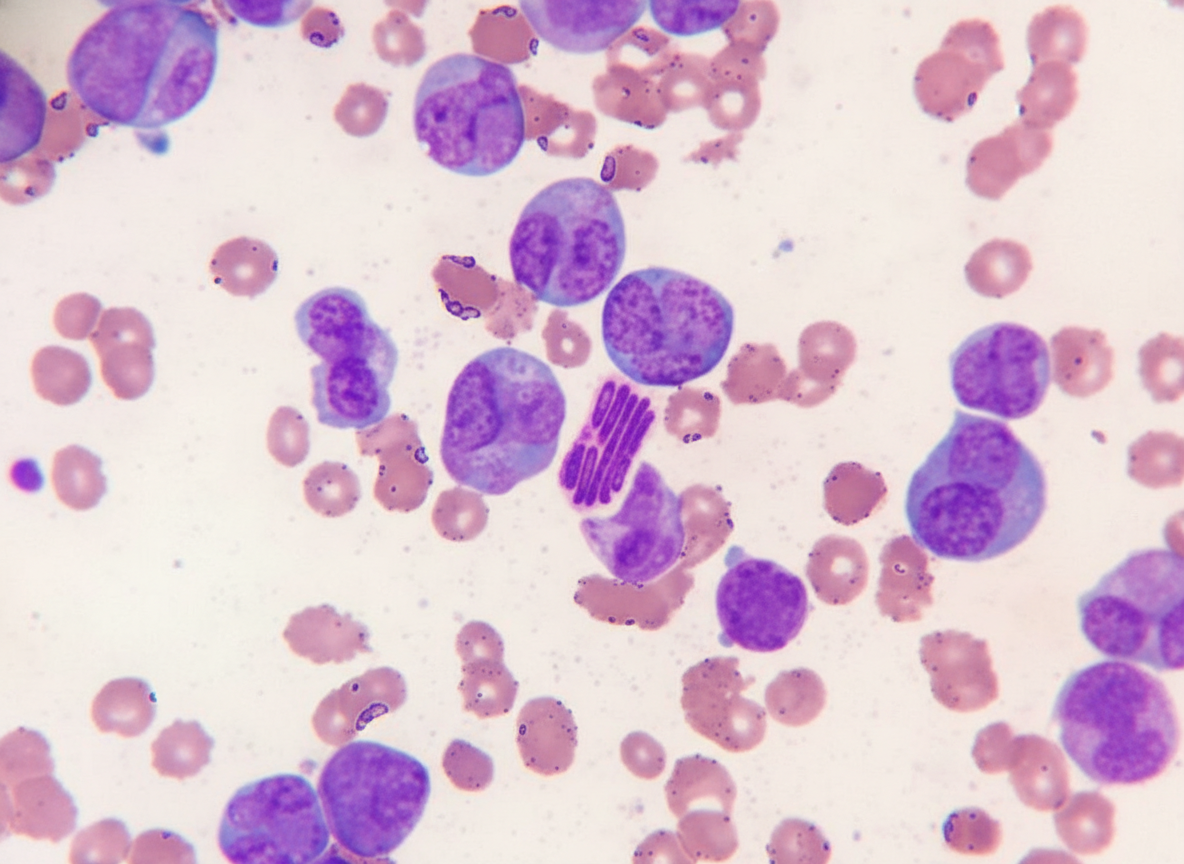
A 45-year-old man presents to the emergency department with fever and easy bruising for 3 days. He has had fatigue for 2 weeks. He has no past medical history, and takes no medications. Excessive bleeding from intravenous lines was reported by the nurse. He does not smoke or drink alcohol. The temperature is 38.2°C (102.6°F), pulse is 105/min, respiration rate is 18/min, and blood pressure is 110/70 mm Hg. On physical examination, he has multiple purpura on the lower extremities and several ecchymoses on the lower back and buttocks. Petechiae are noticed on the soft palate. Cervical painless lymphadenopathy is detected on both sides. The examination of the lungs, heart, and abdomen shows no other abnormalities. The laboratory test results are as follows: Hemoglobin 8 g/dL Mean corpuscular volume 90 μm3 Leukocyte count 18,000/mm3 Platelet count 10,000/mm3 Partial thromboplastin time (activated) 60 seconds Prothrombin time 25 seconds (INR: 2.2) Fibrin split products Positive Lactate dehydrogenase, serum 1,000 U/L A Giemsa-stained peripheral blood smear is shown by the image. Intravenous fluids, blood products, and antibiotics are given to the patient. Based on the most likely diagnosis, which of the following is the best therapy for this patient at this time?
A 30-year-old man comes to the physician for his annual health maintenance examination. The patient has no particular health concerns. He has a history of bilateral cryptorchidism treated with orchidopexy at 8 months of age. This patient is at increased risk for which of the following?
A 35-year-old man presents with a mass on the central part of his neck. He reports it has been growing steadily for the past 2 weeks, and he has also been experiencing fatigue and recurrent fevers. No significant past medical history. The patient denies any smoking history, or alcohol or recreational drug use. He denies any recent travel in the previous 6 months. On physical examination, there are multiple enlarged submandibular and cervical lymph nodes that are firm, mobile, and non-tender. A biopsy of one of the lymph nodes is performed and shows predominantly lymphocytes and histiocytes present in a pattern ‘resembling popcorn’. A flow cytometry analysis demonstrates cells that are CD19 and CD20 positive and CD15 and CD30 negative. Which of the following is the most likely diagnosis in this patient?
A 62-year-old woman presents to her physician with a painless breast mass on her left breast for the past 4 months. She mentions that she noticed the swelling suddenly one day and thought it would resolve by itself. Instead, it has been slowly increasing in size. On physical examination of the breasts, the physician notes a single non-tender, hard, and fixed nodule over left breast. An ultrasonogram of the breast shows a solid mass, and a fine-needle aspiration biopsy confirms the mass to be lobular carcinoma of the breast. When the patient asks about her prognosis, the physician says that the prognosis can be best determined after both grading and staging of the tumor. Based on the current diagnostic information, the physician says that they can only grade, but no stage, the neoplasm. Which of the following facts about the neoplasm is currently available to the physician?
A 57-year-old post-menopausal woman comes to the physician because of intermittent, bloody post-coital vaginal discharge for the past month. She does not have pain with intercourse. Eleven years ago, she had LSIL on a routine Pap smear and testing for high-risk HPV strains was positive. Colposcopy showed CIN 1. She has not returned for follow-up Pap smears since then. She is sexually active with her husband only, and they do not use condoms. She has smoked half a pack of cigarettes per day for the past 25 years and does not drink alcohol. On speculum exam, a 1.4 cm, erythematous exophytic mass with ulceration is noted on the posterior wall of the upper third of the vagina. Which of the following is the most probable histopathology of this mass?
A 55-year-old man comes to the physician because of fatigue and worsening abdominal pain for 4 weeks. He also reports excessive night sweats and a 5.4-kg (12-lb) weight loss during this time. He has a neck swelling for 4 days. Physical examination shows a nontender, enlarged, and fixed supraclavicular lymph node. There is splenomegaly. A CT scan of the thorax and abdomen shows massively enlarged axillary, mediastinal, and cervical lymph nodes. Analysis of an excised cervical lymph node shows lymphocytes with a high proliferative index that stain positive for CD20. Which of the following is the most likely diagnosis?
A 52-year-old woman comes to the physician because of a 6-month history of generalized fatigue, low-grade fever, and a 10-kg (22-lb) weight loss. Physical examination shows generalized pallor and splenomegaly. Her hemoglobin concentration is 7.5 g/dL and leukocyte count is 41,800/mm3. Leukocyte alkaline phosphatase activity is low. Peripheral blood smear shows basophilia with myelocytes and metamyelocytes. Bone marrow biopsy shows cellular hyperplasia with proliferation of immature granulocytic cells. Which of the following mechanisms is most likely responsible for this patient's condition?
Practice by Chapter
Characteristics of benign vs malignant tumors
Practice Questions
Nomenclature of neoplasms
Practice Questions
Carcinogenesis models
Practice Questions
Oncogenes and proto-oncogenes
Practice Questions
Tumor suppressor genes
Practice Questions
DNA repair genes and cancer
Practice Questions
Epigenetic mechanisms in cancer
Practice Questions
Apoptosis and cancer
Practice Questions
Tumor angiogenesis
Practice Questions
Tumor invasion and metastasis
Practice Questions
Carcinogenic agents
Practice Questions
Paraneoplastic syndromes
Practice Questions
Tumor immunology
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app