
Neoplasia — MCQs

On this page
A 55-year-old female presents to her primary care physician complaining of a mass in her mid-thigh. The mass has grown slowly over the past six months and is not painful. The patient’s past medical history is notable for hypertension and hyperlipidemia. She takes lisinopril and rosuvastatin. On examination, there is a firm, immobile mass on the medial aspect of the distal thigh. She has full range of motion and strength in her lower extremities and patellar reflexes are 2+ bilaterally. A biopsy of the mass reveals multiple pleomorphic smooth muscle cells with nuclear atypia. The patient subsequently initiates radiation therapy with plans to undergo surgical resection. This tumor will most strongly stain for which of the following?
A 71-year-old man presents to the primary care clinic with non-specific complaints of fatigue and malaise. His past medical history is significant for diabetes mellitus type II, hypertension, non-seminomatous testicular cancer, and hypercholesterolemia. He currently smokes 1 pack of cigarettes per day, drinks a glass of wine per day, and he currently denies any illicit drug use. His vital signs include: temperature, 36.7°C (98.0°F); blood pressure, 126/74 mm Hg; heart rate, 87/min; and respiratory rate, 17/min. On examination, his physician notices cervical and inguinal lymphadenopathy bilaterally, as well as splenomegaly. The patient comments that he has lost 18.1 kg (40 lb) over the past 6 months without a change in diet or exercise, which he was initially not concerned about. The physician orders a complete blood count and adds on flow cytometry. Based on his age and overall epidemiology, which of the following is the most likely diagnosis?
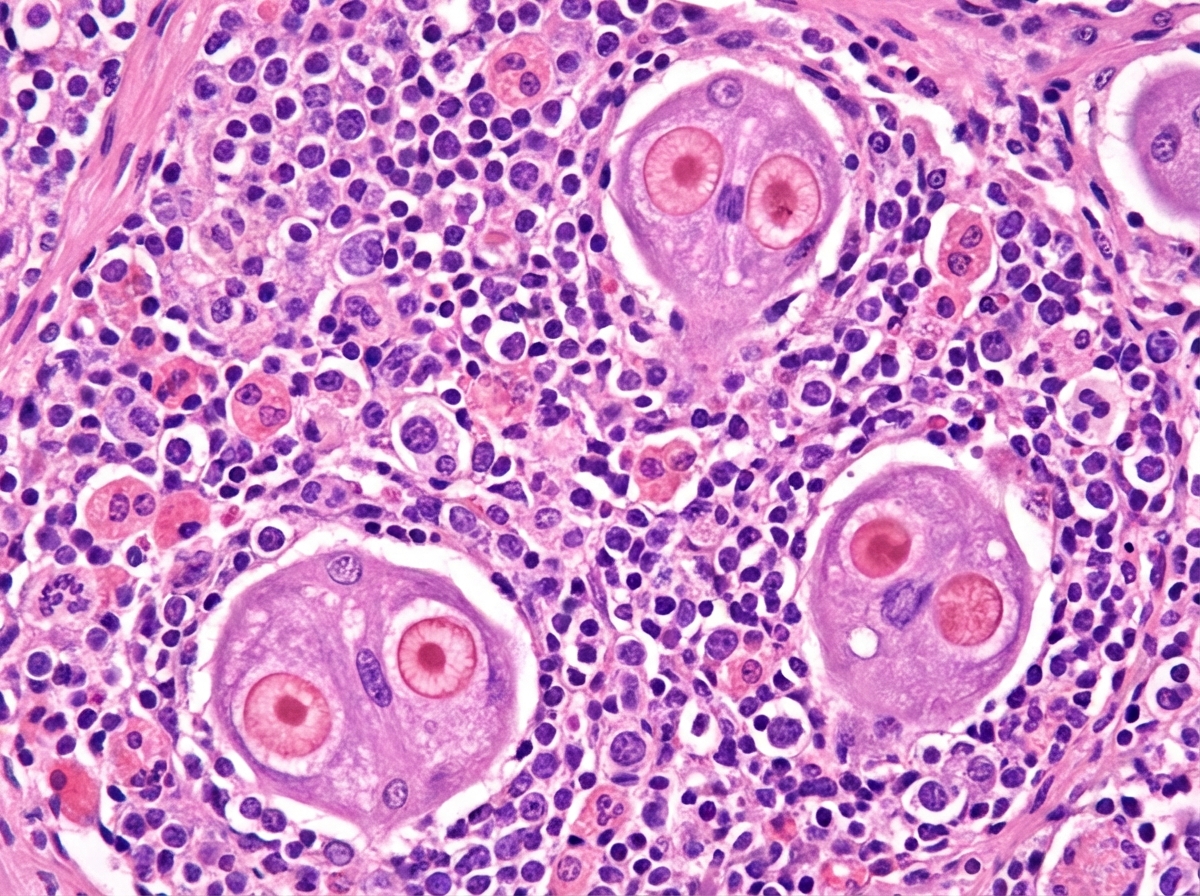
A 53-year-old man comes to the physician for recurring fever and night sweats for the past 6 months. The fevers persist for 7 to 10 days and then subside completely for about a week before returning again. During this period, he has also noticed two painless lumps on his neck that have gradually increased in size. Over the past year, he has had an 8.2-kg (18.1 lbs) weight loss. Two years ago, he had a severe sore throat and fever, which was diagnosed as infectious mononucleosis. He has smoked a pack of cigarettes daily for the past 10 years. He does not drink alcohol. His job involves monthly international travel to Asia and Africa. He takes no medications. His temperature is 39°C (102.2°F), pulse is 90/min, respirations are 22/min, and blood pressure is 105/60 mm Hg. Physical examination shows 2 enlarged, nontender, fixed cervical lymph nodes on each side of the neck. Microscopic examination of a specimen obtained on biopsy of a cervical lymph node is shown. Which of the following additional findings is most likely present in this patient?
A 64-year-old male presents to his primary care physician. Laboratory work-up and physical examination are suggestive of a diagnosis of prostatic adenocarcinoma. A tissue biopsy is obtained, which confirms the diagnosis. Which of the following is indicative of metastatic disease?
A 70-year-old man comes to the physician because of right-sided back pain, red urine, and weight loss for the last 4 months. He has smoked one pack of cigarettes daily for 40 years. A CT scan of the abdomen shows a large right-sided renal mass. Biopsy of the mass shows polygonal clear cells filled with lipids. Which of the following features is necessary to determine the tumor grade in this patient?
A 63-year-old man comes to the physician for the evaluation of a skin lesion on his chest. He first noticed the lesion 2 months ago and thinks that it has increased in size since then. The lesion is not painful or pruritic. He has type 2 diabetes mellitus, hypercholesterolemia, and glaucoma. The patient has smoked 1 pack of cigarettes daily for the last 40 years and drinks two to three beers on the weekend. Current medications include metformin, atorvastatin, topical timolol, and a multivitamin. Vital signs are within normal limits. The lesion is partly elevated on palpation and does not change its form on pinching. Examination reveals an asymmetric lesion with irregular borders, variegated pigmentation (areas of brown, black, red, and violaceous coloration), and a diameter greater than 1 cm. A photograph of the lesion is shown. Which of the following is the most likely diagnosis?

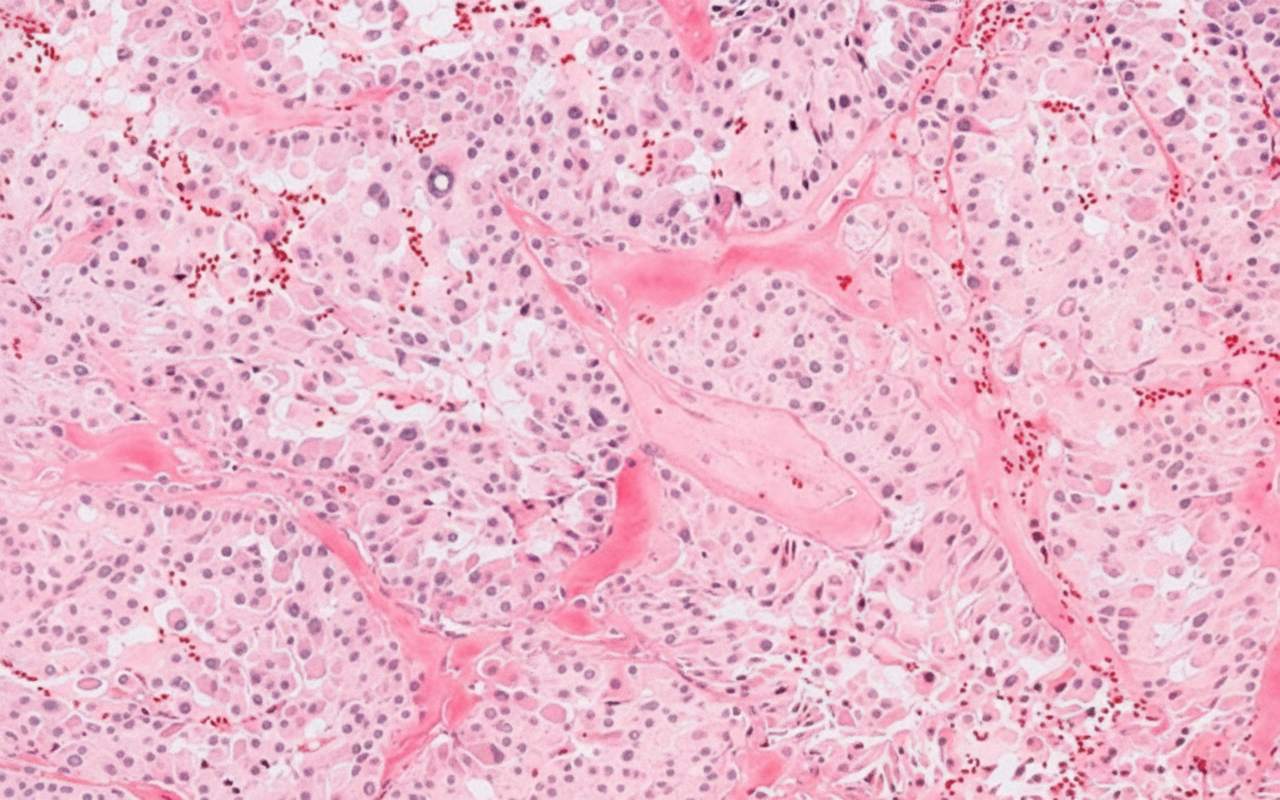
A 45-year old man comes to the physician because of a painless neck lump and a 2-month history of difficulty swallowing. He has a history of recurrent nephrolithiasis and episodic hypertension. Physical examination shows a 3 × 3-cm, nontender nodule at the level of the thyroid cartilage. A photomicrograph of a section of tissue obtained by core needle biopsy of the nodule is shown. Which of the following is the most likely diagnosis?
A newborn of a mother with poor antenatal care is found to have a larger than normal head circumference with bulging fontanelles. Physical examination reveals a predominant downward gaze with marked eyelid retraction and convergence-retraction nystagmus. Ultrasound examination showed dilated lateral ventricles and a dilated third ventricle. Further imaging studies reveal a solid mass in the pineal region. Which of the following is the most likely underlying pathophysiological mechanism responsible for the neurological signs in this patient?
A 65-year-old man presents with painless swelling of the neck over the past week. He also has noted severe night sweats, which require a change of clothes and bed linens the next day. His medical history is significant for long-standing hypertension. He received a kidney transplant 6 years ago. His current medications include amlodipine, metoprolol, furosemide, aspirin, tacrolimus, and mycophenolate. His family history is significant for his sister, who died last year from lymphoma. A review of systems is positive for a 6-kg (13.2-lb) unintentional weight loss over the past 2 months. His vital signs include: temperature 37.8°C (100.0°F) and blood pressure 120/75 mm Hg. On physical examination, there are multiple painless lymph nodes, averaging 2 cm in diameter, palpable in the anterior and posterior triangles of the neck bilaterally. Axillary and inguinal lymphadenopathy is palpated on the right side. Abdominal examination is significant for a spleen of 16 cm below the costal margin on percussion. Laboratory studies are significant for the following: Hemoglobin 9 g/dL Mean corpuscular volume 88 μm3 Leukocyte count 12,000/mm3 Platelet count 130,000/mm3 Creatinine 1.1 mg/dL Lactate dehydrogenase (LDH) 1,000 U/L A peripheral blood smear is unremarkable. Which of the following is the most likely diagnosis in this patient?
A 61-year-old woman presents to her primary care physician for a routine check-up. Physical examination demonstrates asymmetric peripheral neuropathy in her feet. The patient has no previous relevant history and denies any symptoms of diabetes. Routine blood work shows normal results, and she is referred to a hematologist. Subsequent serum protein electrophoresis demonstrates a slightly elevated gamma globulin level, and monoclonal gammopathy of undetermined significance is diagnosed. Which of the following diseases is most likely to develop over the course of this patient’s condition?
Practice by Chapter
Characteristics of benign vs malignant tumors
Practice Questions
Nomenclature of neoplasms
Practice Questions
Carcinogenesis models
Practice Questions
Oncogenes and proto-oncogenes
Practice Questions
Tumor suppressor genes
Practice Questions
DNA repair genes and cancer
Practice Questions
Epigenetic mechanisms in cancer
Practice Questions
Apoptosis and cancer
Practice Questions
Tumor angiogenesis
Practice Questions
Tumor invasion and metastasis
Practice Questions
Carcinogenic agents
Practice Questions
Paraneoplastic syndromes
Practice Questions
Tumor immunology
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app