
Neoplasia — MCQs

On this page
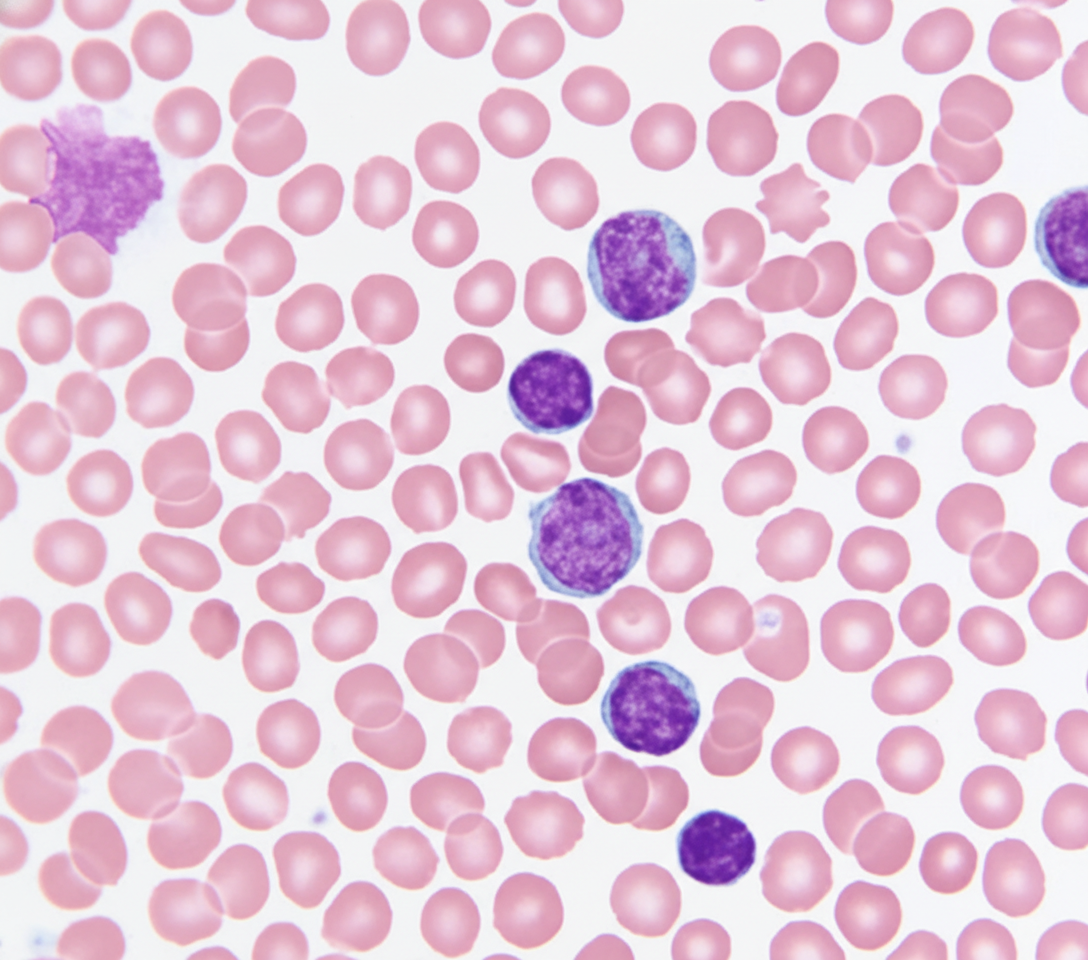
A 69-year-old Caucasian man presents for a routine health maintenance examination. He feels well. He has no significant past medical history. He takes aspirin for the occasional headaches that he has had for over several years. He exercises every day and does not smoke. His father was diagnosed with a hematologic malignancy at 79 years old. The patient’s vital signs are within normal limits. Physical examination shows no abnormalities. The laboratory test results are as follows: Hemoglobin 14.5 g/dL Leukocyte count 62,000/mm3 Platelet count 350,000/mm3 A peripheral blood smear is obtained (shown on the image). Which of the following best explains these findings?
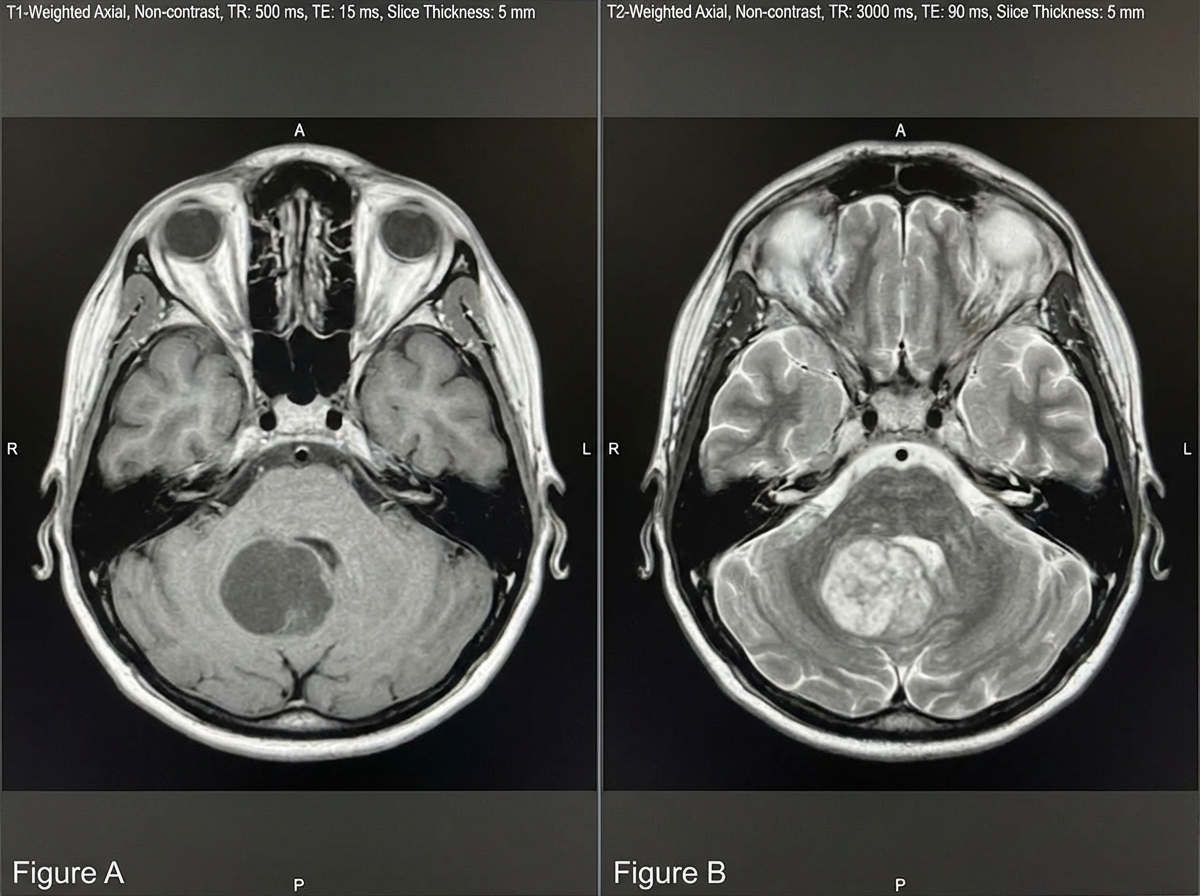
A 6-year-old boy is brought in by his mother to his pediatrician for headache and nausea. His headaches began approximately 3 weeks ago and occur in the morning. Throughout the 3 weeks, his nausea has progressively worsened, and he had 2 episodes of emesis 1 day ago. On physical exam, cranial nerves are grossly intact, and his visual field is intact. The patient has a broad-based gait and difficulty with heel-to-toe walking, as well as head titubation. Fundoscopy demonstrates papilledema. A T1 and T2 MRI of the brain is demonstrated in Figures A and B, respectively. Which of the following is most likely the diagnosis?
A 55-year-old male presents with complaints of intermittent facial flushing. He also reports feeling itchy after showering. On review of systems, the patient says he has been having new onset headaches recently. On physical exam, his vital signs, including O2 saturation, are normal. He has an abnormal abdominal mass palpable in the left upper quadrant. A complete blood count reveals: WBCs 6500/microliter; Hgb 18.2 g/dL; Platelets 385,000/microliter. Which of the following is most likely responsible for his presentation?
A 53-year-old man is being evaluated for a 3-week history of fatigue, difficulty to concentrate, dyspnea with exertion, dizziness, and digital pain that improves with cold. He has smoked half a pack of cigarettes a day since he was 20. His current medical history involves hypertension. He takes enalapril daily. The vital signs include a blood pressure of 131/82 mm Hg, a heart rate of 95/min, and a temperature of 36.9°C (98.4°F). On physical examination, splenomegaly is found. A complete blood count reveals thrombocytosis of 700,000 cells/μL. Lab work further shows decreased serum iron, iron saturation, and serum ferritin and increased total iron binding capacity. A blood smear reveals an increased number of abnormal platelets, and a bone marrow aspirate confirmed the presence of dysplastic megakaryocytes. A mutation on his chromosome 9 confirms the physician's suspicion of a certain clonal myeloproliferative disease. The patient is started on hydroxyurea. What is the most likely diagnosis?
A 43-year-old woman presents to your clinic for the evaluation of an abnormal skin lesion on her forearm. The patient is worried because her mother passed away from melanoma. You believe that the lesion warrants biopsy for further evaluation for possible melanoma. Your patient is concerned about her risk for malignant disease. What is the most important prognostic factor of melanoma?
An investigator studying targeted therapy in patients with gastrointestinal stromal tumors requires a reliable test to determine the spatial distribution of CD117-positive cells in biopsy specimens. Which of the following is the most appropriate test?
A 70-year-old man presents to his physician for evaluation of fullness and swelling of the left side of the abdomen over the last month. During this time, he has had night sweats and lost 2 kg (4.4 lb) unintentionally. He has no history of severe illness and takes no medications. The vital signs include: blood pressure 115/75 mm Hg, pulse 75/min, and temperature 36.8℃ (98.2℉). The abdomen has asymmetric distention. Percussion and palpation of the left upper quadrant reveal splenomegaly. No lymphadenopathy is detected. Heart and lung examination shows no abnormalities. The laboratory studies show the following: Hemoglobin 9.5 g/dL Mean corpuscular volume 95 μm3 Leukocyte count 8,000/mm3 Platelet count 240,000/mm3 Ultrasound shows a spleen size of 15 cm, mild hepatomegaly, and mild ascites. The peripheral blood smear shows teardrop-shaped and nucleated red blood cells (RBCs) and immature myeloid cells. Marrow is very difficult to aspirate but reveals hyperplasia of all 3 lineages. The tartrate-resistant acid phosphatase (TRAP) test is negative. The cytogenetic analysis is negative for translocation between chromosomes 9 and 22. Which of the following laboratory findings is most likely to be present in this patient?
A 59-year-old woman comes to the physician because of a 2-month history of fatigue and abdominal discomfort. Over the past 6 months, she has had a 5.4-kg (12-lb) weight loss. She takes no medications. Her temperature is 37.8°C (100°F), pulse is 70/min, respirations are 13/min, and blood pressure is 125/80 mm Hg. Cardiopulmonary examination shows no abnormalities. The spleen is palpated 3 cm below the left costal margin. Laboratory studies show: Hemoglobin 9.4 g/dL Mean corpuscular volume 86 μm3 Leukocyte count 58,000/mm3 Segmented neutrophils 54% Bands 8% Lymphocytes 7% Myelocytes 5% Metamyelocytes 10% Promyelocytes 4% Blasts 5% Monocytes 1% Eosinophils 4% Basophils 2% Platelet count 850,000/mm3 Serum Creatinine 0.9 mg/dL LDH 501 U/L Bone marrow biopsy shows hyperplastic myelopoiesis with granulocytosis. Which of the following is the most appropriate next step in management?
An 11-year-old boy is brought to the pediatrician by his mother for vomiting. The patient has been vomiting for the past week, and his symptoms have not been improving. His symptoms are worse in the morning and tend to improve throughout the day. The patient also complains of occasional headaches and had diarrhea several days ago. The patient eats a balanced diet and does not drink soda or juice. The patient's brothers both had diarrhea recently that resolved spontaneously. His temperature is 99.5°F (37.5°C), blood pressure is 80/45 mmHg, pulse is 90/min, respirations are 16/min, and oxygen saturation is 98% on room air. On physical exam, the patient appears to be in no acute distress. Cardiopulmonary exam reveals a minor flow murmur. Neurological exam reveals cranial nerves II-XII as grossly intact with mild narrowing of the patient's visual fields. The patient's gait is stable, and he is able to jump up and down. Which of the following is the most likely direct cause of this patient's presentation?
A 24-year-old man is brought to the physician because of increasing pain and swelling of the left knee for 2 months. The pain has awoken him from his sleep on multiple occasions. He tried ibuprofen but has had no relief of his symptoms. There is no family or personal history of serious illness. Vital signs are within normal limits. On examination, the left knee is mildly swollen and tender; range of motion is limited by pain. An x-ray of the left knee is shown. Which of the following is the most likely diagnosis?

Practice by Chapter
Characteristics of benign vs malignant tumors
Practice Questions
Nomenclature of neoplasms
Practice Questions
Carcinogenesis models
Practice Questions
Oncogenes and proto-oncogenes
Practice Questions
Tumor suppressor genes
Practice Questions
DNA repair genes and cancer
Practice Questions
Epigenetic mechanisms in cancer
Practice Questions
Apoptosis and cancer
Practice Questions
Tumor angiogenesis
Practice Questions
Tumor invasion and metastasis
Practice Questions
Carcinogenic agents
Practice Questions
Paraneoplastic syndromes
Practice Questions
Tumor immunology
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app