
Neoplasia — MCQs

On this page
A 16-year-old male presents to the emergency department complaining of episodes of pounding headache, chest fluttering, and excessive sweating. He has a past history of kidney stones that are composed of calcium oxalate. He does not smoke or drink alcohol. Family history reveals that his mother died of thyroid cancer. Vital signs reveal a temperature of 37.1°C (98.7°F), blood pressure of 200/110 mm Hg and pulse of 120/min. His 24-hour urine calcium, serum metanephrines, and serum normetanephrines levels are all elevated. Mutation of which of the following genes is responsible for this patient's condition?
A 38-year-old man presents to his primary care practitioner for 2 months of rectal bleeding. He also reports occasional diarrhea and abdominal pain. His family history is relevant for his father and uncle, who died from complications of colorectal cancer. Colonoscopy shows more than 10 colorectal adenomas. Which of the following genes is most likely affected in this patient?
A 72-year-old man presents to the emergency department with a complaint of rectal bleeding. He describes blood mixed in with the stool, which is associated with a change in his normal bowel habit such that he is going more frequently than normal. He also has some crampy left-sided abdominal pain and weight loss. His symptoms started 2 months ago, but he thought they are due to lack of dietary fiber intake and excess consumption of red meat. He has had type 2 diabetes mellitus for 35 years for which he takes metformin. He also uses daily low-dose aspirin for cardioprotection and occasional naproxen for knee pain. His family history is irrelevant. On examination, his abdomen and digital rectal examination are normal. Colonoscopy shows an ulcerating mucosal lesion with a narrow bowel lumen and biopsy shows a moderately differentiated adenocarcinoma. Which of the following is the greatest risk factor for colorectal cancer in this patient?
A 62-year-old man seeks evaluation at an outpatient clinic for a single, red, crusty lesion on the shaft of his penis and a similar lesion on the middle finger of his left hand. He recently immigrated to the US from Africa. The lesions are painless and the physicians in his country treated him for syphilis and eczema, with no improvement. He lives with his 4th wife. He smokes 2 packs of cigarette per day and has been doing so for the last 30 years. He is not aware of any family members with malignancies or hereditary diseases. The physical examination is remarkable for an erythematous plaque, with areas of crusting, oozing, and irregular borders on the dorsal surface of the penile shaft and a similar lesion on his left middle finger (shown in the picture). The regional lymph nodes are not affected. A biopsy is obtained and the pathologic evaluation reveals cells with nuclear hyperchromasia, multinucleation, and increased mitotic figures within the epidermis. What is the most likely diagnosis?

A 35-year-old woman, gravida 2, para 2, comes to the physician with intermenstrual bleeding and heavy menses for the past 4 months. She does not take any medications. Her father died of colon cancer at the age of 42 years. A curettage sample shows dysplastic tall, columnar, cells in the endometrium without intervening stroma. Germline sequencing shows a mutation in the MLH1 gene. Which of the following is the most likely underlying cause of neoplasia in this patient?
A 45-year-old woman presents with heavy menstrual bleeding between her periods. The patient also complains of experiencing an irregular menstrual cycle, weight loss, bloating, and constipation. She has had 3 uncomplicated pregnancies, all of which ended with normal vaginal deliveries at term. She has never taken oral contraception, and she does not take any medication at the time of presentation. She has no family history of any gynecological malignancy; however, her grandfather and mother had colon cancer that was diagnosed before they turned 50. On physical examination, the patient appears pale. Gynecological examination reveals a bloody cervical discharge and slight uterine enlargement. Endometrial biopsy reveals endometrial adenocarcinoma. Colonoscopy reveals several polyps located in the ascending colon, which are shown to be adenocarcinomas on histological evaluation. Which of the following mechanisms of DNA repair is likely to be disrupted in this patient?
A 41-year-old man with HIV comes to the physician because of rectal bleeding and itching for 2 weeks. During this period, he has also had pain with defecation. Four months ago, he was diagnosed with anogenital warts that were treated with cryotherapy. Over the past year, he has been sexually active with 3 male partners. He uses condoms inconsistently. Current medications are zidovudine, emtricitabine, and efavirenz. Digital rectal examination and anoscopy show an exophytic mass on the anal margin that is protruding into the anal canal. The mass is tender to palpation and bleeds easily on contact. Laboratory studies show a leukocyte count of 7,600/mm3 and a CD4+ T-lymphocyte count of 410/mm3 (N ≥ 500). A biopsy specimen of the lesion shows a well-differentiated squamous cell carcinoma. Which of the following cellular processes was most likely involved in the pathogenesis of this patient's malignancy?
A 5-year-old male is brought to his pediatrician after recurrent, prolonged upper respiratory infections over a period of several months. Physical exam reveals petechiae on the patient's legs and arms. Laboratory studies show hemoglobin: 10 g/dL, platelet count: 35,000/mm^3, leukocyte count: 6,600/mm^3. A bone marrow aspiration shows an abundance of lymphoblasts indicative of acute lymphoblastic leukemia (ALL). Positive immunostaining for which of the following would support a diagnosis of precursor B-cell leukemia?
A 65-year-old man comes to the physician for evaluation of a neck mass and weight loss. He first noticed the growing mass 2 months ago. The mass is not painful. He also has decreased appetite and intermittent abdominal pain. He has lost 10 kg (22 lb) of weight over the past 3 months. Sometimes, he wakes up in the morning drenched in sweat. He takes daily over-the-counter multivitamins. He appears pale. His pulse is 65/min, blood pressure is 110/70 mm Hg, and temperature is 38.1°C (100.6°F). Physical exam shows a painless, golf ball-sized mass in the anterior triangle of the neck. A biopsy shows large cells with a bilobed nucleus that are CD15-positive and CD30-positive. Laboratory analysis of serum shows a calcium level of 14.5 mg/dL and a parathyroid hormone level of 40 pg/mL. Which of the following is the most likely explanation of this patient's laboratory findings?
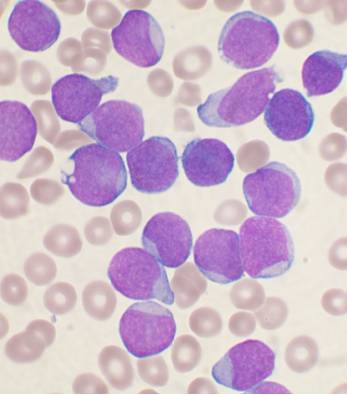
A 7-year-old boy presents to the ER with progressive dysphagia over the course of 3 months and a new onset fever for the past 24 hours. The temperature in the ER was 39.5°C (103.1°F). There are white exudates present on enlarged tonsils (Grade 2). Routine blood work reveals a WBC count of 89,000/mm3, with the automatic differential yielding a high (> 90%) percentage of lymphocytes. A peripheral blood smear is ordered, demonstrating the findings in the accompanying image. The peripheral smear is submitted to pathology for review. After initial assessment, the following results are found on cytologic assessment of the cells: TdT: positive CALLA (CD 10): positive Which of the following cell markers are most likely to be positive as well?
Practice by Chapter
Characteristics of benign vs malignant tumors
Practice Questions
Nomenclature of neoplasms
Practice Questions
Carcinogenesis models
Practice Questions
Oncogenes and proto-oncogenes
Practice Questions
Tumor suppressor genes
Practice Questions
DNA repair genes and cancer
Practice Questions
Epigenetic mechanisms in cancer
Practice Questions
Apoptosis and cancer
Practice Questions
Tumor angiogenesis
Practice Questions
Tumor invasion and metastasis
Practice Questions
Carcinogenic agents
Practice Questions
Paraneoplastic syndromes
Practice Questions
Tumor immunology
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app