
Neoplasia — MCQs

On this page
A 22-year-old woman comes to the physician because of hearing loss and unsteadiness while standing and walking for the past 2 months. She needs support from a wall to prevent herself from falling. She has not had any recent injuries and has no history of serious illness. Vital signs are within normal limits. Examination shows an unsteady gait. She sways when asked to stand upright with her feet together. She is unable to hear fingers rubbing next to her ears or repeat words whispered in her ears bilaterally. An MRI of the brain shows a 3-cm tumor in the right cerebellopontine angle and a 4.5-cm tumor in the left cerebellopontine angle. This patient is most likely to develop which of the following in the future?
A 42-year-old woman presents to her primary care physician with fatigue. She reports that over the past 2 months, she has felt increasingly tired despite no changes in her diet or exercise. Her past medical history is notable for obesity, seasonal allergies, and hypertension. She takes ranitidine as needed and hydrochlorothiazide daily. Her family history is notable for colorectal cancer in her mother and maternal uncle, endometrial cancer in her maternal aunt, and ovarian cancer in her maternal grandmother. Her temperature is 98.8°F (37.1°C), blood pressure is 132/71 mmHg, pulse is 89/min, and respirations are 17/min. On exam, she has conjunctival pallor. A stool sample is hemoccult positive. A colonoscopy reveals a fungating hemorrhagic mass in the ascending colon. Which of the following processes is likely impaired in this patient?
A 65-year-old man with a 40-pack-year smoking history presents with hemoptysis and a persistent cough. Chest CT shows a 3.5 cm centrally located mass in the right main bronchus. Positron emission tomography confirms a malignant nodule. Bronchoscopy with transbronchial biopsy is performed and a specimen sample of the nodule is sent for frozen section analysis. The tissue sample is most likely to show which of the following tumor types?
A 70-year-old man is brought to the emergency department by his wife because of progressive confusion for the past 2 weeks. He has also had a 4.5-kg (10-lb) weight loss and fatigue during the last 6 months. Physical examination shows enlarged lymph nodes in the right axilla and faint expiratory wheezing in the right middle lung field. He is only oriented to person. Serum studies show a sodium concentration of 125 mEq/L and increased antidiuretic hormone concentration. An x-ray of the chest shows a right-sided hilar mass with mediastinal fullness. A biopsy of the hilar mass is most likely to show cells that stain positive for which of the following?
A 61-year-old male presents to the ER with abdominal discomfort and malaise over the past 2 weeks. He states he is married and monogamous. He has a temperature of 39.4°C (102.9°F) and complains of night sweats as well. On physical exam, he has an enlarged spleen with mild tenderness and pale nail beds. There is mild tonsillar erythema and the pulmonary exam demonstrates scattered crackles. A complete blood count demonstrates anemia, thrombocytopenia, and leukocytosis with lymphocytic predominance. A bone marrow aspiration is scheduled the next morning based on the peripheral blood smear findings but was inconclusive due to a low yield. The patient was admitted to the hospital due to the anemia and given a transfusion of packed red blood cells and wide spectrum antibiotics. He is released home the next day with instructions for primary care follow-up. Which of the following laboratory findings is most reliably positive for the primary cause of this illness?
A 4-year-old girl is brought to the physician because of a 3-week history of generalized fatigue and easy bruising. During the past week, she has also had fever and severe leg pain that wakes her up at night. Her temperature is 38.3°C (100.9°F), pulse is 120/min, and respirations are 30/min. Examination shows cervical and axillary lymphadenopathy. The abdomen is soft and nontender; the liver is palpated 3 cm below the right costal margin, and the spleen is palpated 2 cm below the left costal margin. Laboratory studies show: Hemoglobin 10.1 g/dL Leukocyte count 63,000/mm3 Platelet count 27,000/mm3 A bone marrow aspirate predominantly shows immature cells that stain positive for CD10, CD19, and TdT. Which of the following is the most likely diagnosis?
A 71-year-old African American man with a history of prostatic adenocarcinoma presents to his oncologist with low back pain. He was diagnosed with non-resectable prostatic adenocarcinoma 4 years ago. He has undergone radiation therapy and chemotherapy. Over the past 3 months, he has developed constant mild non-radiating low back pain that occasionally wakes him up from sleep. He denies any recent falls or trauma. His past medical history is notable for hypertension, diabetes mellitus, coronary artery disease, and gout. He also has a history of thyroid cancer and underwent thyroidectomy 5 years ago. He takes lisinopril, metoprolol, aspirin, metformin, and allopurinol. He has a 40-pack-year smoking history and drinks alcohol socially. His temperature is 99.2°F (37.3°C), blood pressure is 150/85 mmHg, pulse is 84/min, and respirations are 18/min. On exam, he is well-appearing and in no acute distress. He is mildly tender to palpation along the lumbar vertebral spinous processes. A computerized tomography (CT) scan of the lumbar spine demonstrates a blastic and sclerotic lesion in the L5 vertebral body. Which of the following findings would most likely be seen on a serum study of this patient?
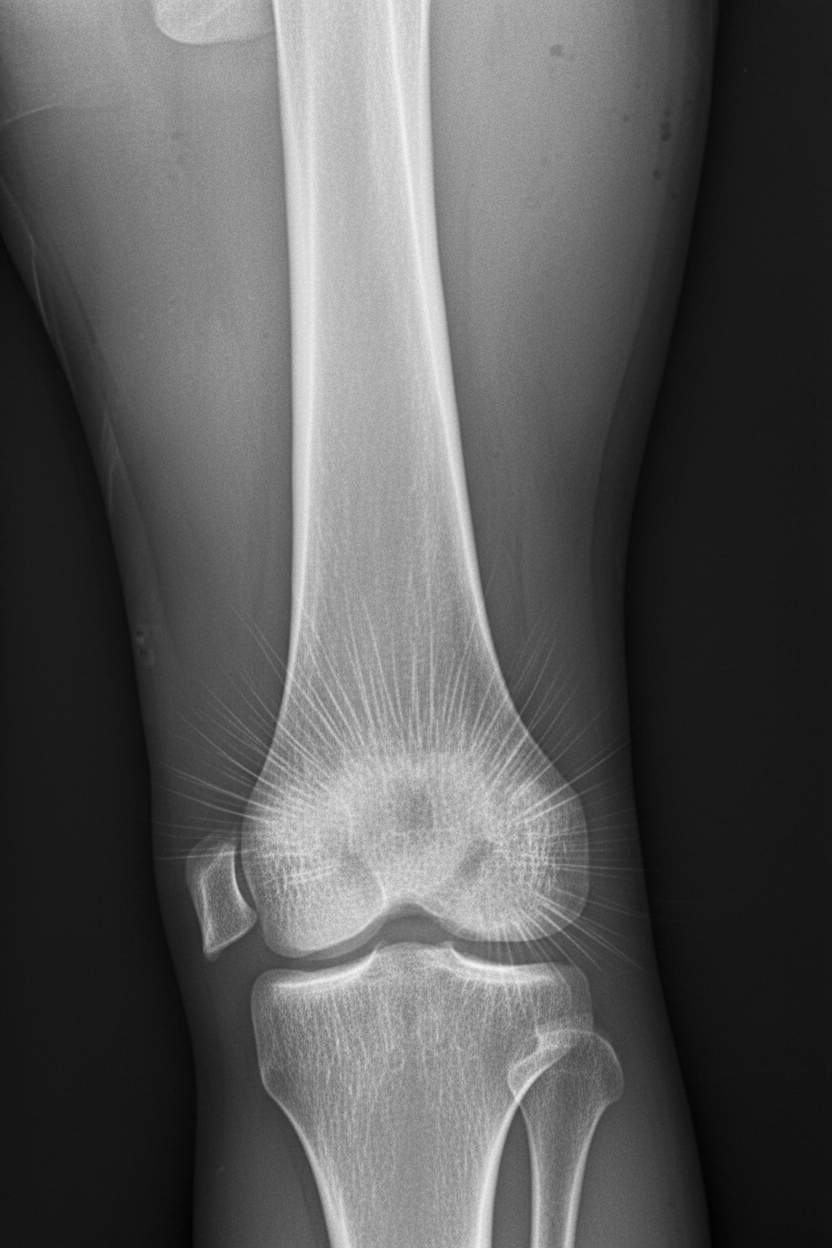
A 13-year-old boy is brought to his pediatrician for evaluation of leg pain. Specifically, he has been having pain around his right knee that has gotten progressively worse over the last several months. On presentation, he has swelling and tenderness over his right distal femur. Radiographs are obtained and the results are shown in figure A. His family history is significant in that several family members also had this disorder and others had pathology in the eye near birth. The patient is referred for a genetic consult, and a mutation is found on a certain chromosome. The chromosome that is most likely affected also contains a gene that is associated with which of the following pathologies?
A 32-year-old woman visits her primary care provider with the results of a recent colonoscopy, which was ordered after 3 episodes of rectal bleeding in the last month. Her grandmother, mother, and sister all have been diagnosed with nonpolyposis colorectal cancer, at ages 65, 50, and 40 years, respectively. Colonoscopy for this patient revealed a large, flat, right-sided adenoma. Histopathological examination of the lesion showed villous histology and high-grade dysplasia. Which of the following helps explain the condition of this patient?
A 58-year-old male undergoes a surveillance colonoscopy in which a 2 cm adenoma is identified and removed. Had this adenoma not been excised, the patient would have been at risk of progression to carcinoma. Which of the following is the final mutational step in the progression from adenoma to carcinoma?
Practice by Chapter
Characteristics of benign vs malignant tumors
Practice Questions
Nomenclature of neoplasms
Practice Questions
Carcinogenesis models
Practice Questions
Oncogenes and proto-oncogenes
Practice Questions
Tumor suppressor genes
Practice Questions
DNA repair genes and cancer
Practice Questions
Epigenetic mechanisms in cancer
Practice Questions
Apoptosis and cancer
Practice Questions
Tumor angiogenesis
Practice Questions
Tumor invasion and metastasis
Practice Questions
Carcinogenic agents
Practice Questions
Paraneoplastic syndromes
Practice Questions
Tumor immunology
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app