
Neoplasia — MCQs

On this page
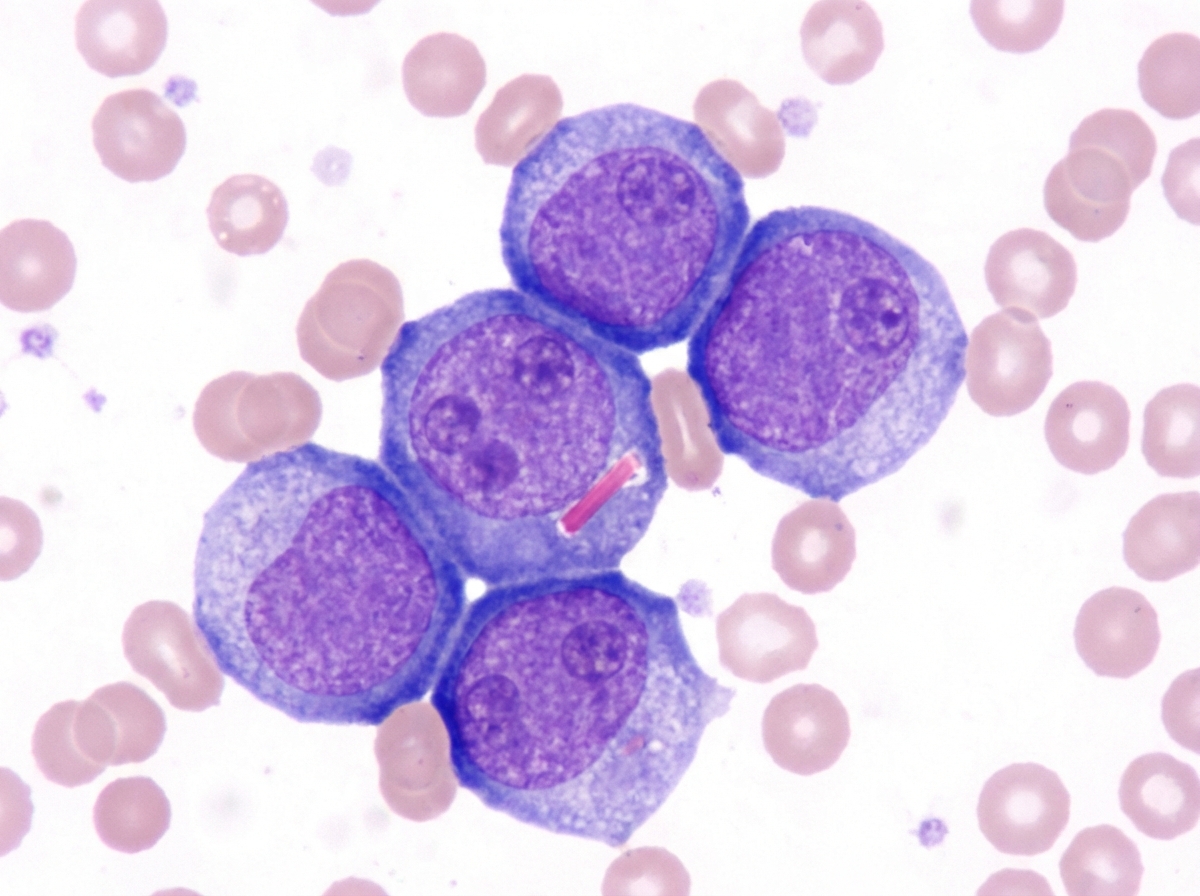
A 67-year-old man comes to the physician because of a 2-month history of generalized fatigue. On examination, he appears pale. He also has multiple pinpoint, red, nonblanching spots on his extremities. His spleen is significantly enlarged. Laboratory studies show a hemoglobin concentration of 8.3 g/dL, a leukocyte count of 81,000/mm3, and a platelet count of 35,600/mm3. A peripheral blood smear shows immature cells with large, prominent nucleoli and pink, elongated, needle-shaped cytoplasmic inclusions. Which of the following is the most likely diagnosis?
A 40-year-old woman residing at an iodine-deficient endemic area presents to the physician with a painless and gradually progressive anterior neck mass. She has occasional dysphagia, but has no history of prior head and neck irradiation. The examination shows a mass that moves with deglutition, suggesting a thyroid mass. An ultrasound of the neck reveals a 3 cm x 3 cm (1.2 in x 1.2 in) mass in the right thyroid lobe with punctate microcalcifications, hypoechogenicity, irregular margins, and enhanced vascularity. There is no cervical lymphadenopathy. Her serum TSH is 3.3 mU/L, serum T3 is 2.2 nmol/L, and serum T4 is 111 nmol/L. An FNAC of the nodule shows abundant follicular cells suspicious of follicular neoplasm. A right lobectomy with isthmectomy is performed. Which of the following histopathological finding is diagnostic?
A 24-year-old woman complains of intermittent fever and joint pain. She says that these symptoms have been present for the past month. Before that, she had no signs or symptoms and was completely healthy. She has also lost her appetite and some weight. A complete blood count (CBC) showed severe pancytopenia. What is the next best step in evaluating this patient?
A 75-year-old female comes to the physician’s office with complaints of right lower quadrant pain. She has been experiencing these symptoms for the last 6 months and they have progressively gotten worse. An ultrasound reveals a large ovarian mass and abdominal and pelvic CT reveals no metastases. Her serum levels of CA-125 are elevated and the biopsy reveals the primary neoplasm as ovarian in origin. Her cancer is characterized as invasive carcinoma without metastasis. Which of the following cellular changes is consistent with this diagnosis?
A 49-year-old woman presents to her physician with complaints of breast swelling and redness of the skin over her right breast for the past 1 month. She also mentions that the skin above her right breast appears to have thickened. She denies any pain or nipple discharge. The past medical history is significant for a total abdominal hysterectomy at 45 years of age. Her last mammogram 1 year ago was negative for any pathologic changes. On examination, the right breast was diffusely erythematous with gross edema and tenderness and appeared larger than the left breast. The right nipple was retracted and the right breast was warmer than the left breast. No localized mass was palpated. Which of the following statements best describes the patient’s most likely condition?
A 57-year-old woman comes to the physician because of a 1-month history of multiple swellings in both her axillae. She says they are generally painless, but are sometimes painful on the weekends. She also has increased fatigue, recurring low-grade fevers, and generalized pruritus. She does not smoke. She drinks five to six beers on the weekends. Her temperature is 37°C (98.6°F), pulse is 80/min, respirations are 12/min, and blood pressure is 130/70 mm Hg. Physical examination reveals multiple firm and nontender axillary lymph nodes. A lymph node biopsy shows multinucleate giant lymphocytes with prominent nucleoli that resemble eosinophilic inclusions. Which of the following additional findings would be associated with a poor prognosis in this patient?
A 70-year-old woman presents with a 2-week history of severe fatigue. Over the past month, she has unintentionally lost 2 kg (4.4 lb). Three years ago, she was diagnosed with myelodysplastic syndrome. Currently, she takes no medications other than aspirin for occasional knee pain. She does not smoke or drink alcohol. Her vital signs are within the normal range. On physical examination, her conjunctivae are pale. Petechiae are present on the distal lower extremities and on the soft and hard palates. Palpation reveals bilateral painless cervical lymphadenopathy. Examination of the lungs, heart, and abdomen shows no abnormalities. Laboratory studies show: Hemoglobin 9 g/dL Mean corpuscular volume 90 μm3 Leukocyte count 3000/mm3 Platelet count 20,000/mm3 A Giemsa-stained peripheral blood smear is shown in the image. Which of the following best explains these findings?
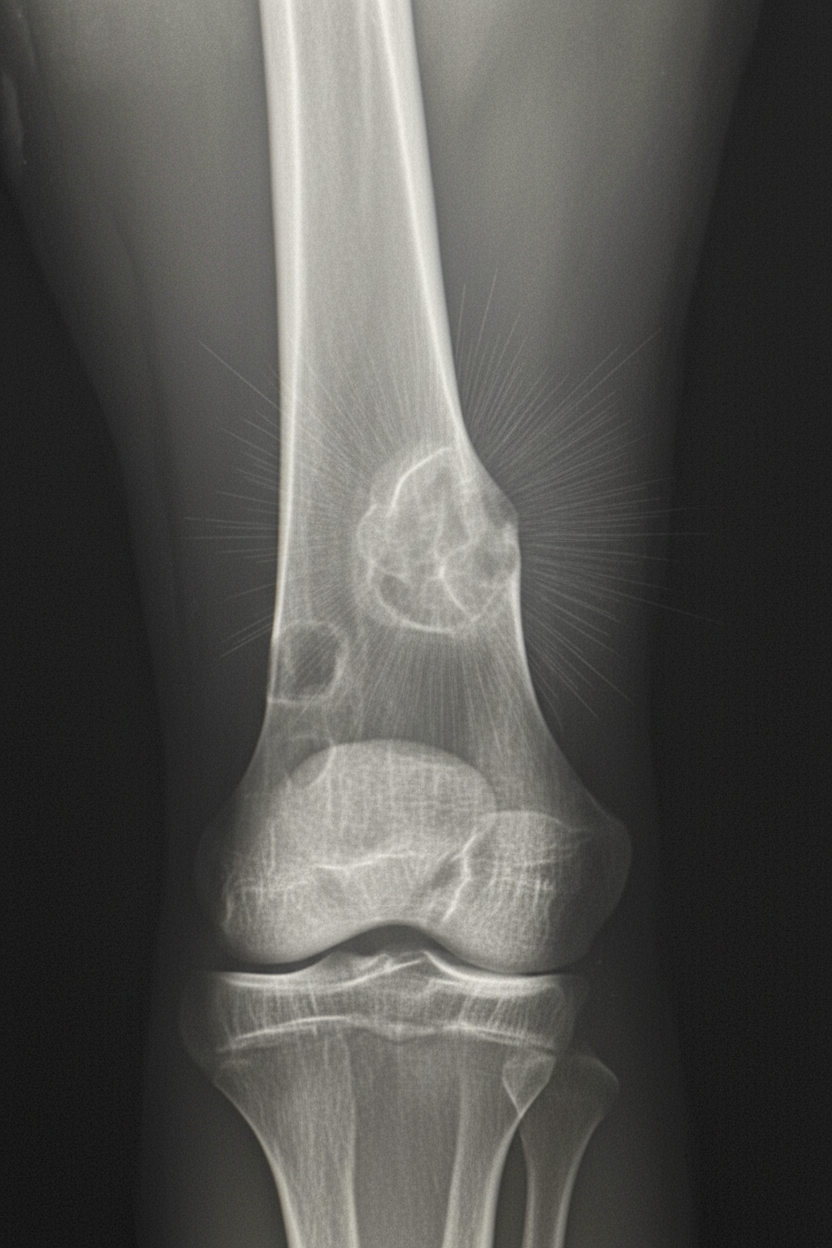
A 17-year-old boy is brought to the physician because of progressive right knee pain for the past 3 months. He reports that the pain is worse at night and while doing sports at school. He has not had any trauma to the knee or any previous problems with his joints. His vital signs are within normal limits. Examination of the right knee shows mild swelling and tenderness without warmth or erythema; the range of motion is limited. He walks with an antalgic gait. Laboratory studies show an alkaline phosphatase of 180 U/L and an erythrocyte sedimentation rate of 80 mm/h. An x-ray of the right knee is shown. Which of the following is the most likely diagnosis?
A 6-year-old boy presents to your office with loss of his peripheral vision. His mother discovered this because he was almost struck by a vehicle that "he couldn't see at all". In addition, he has been complaining of a headache for the last several weeks and had an episode of vomiting 2 days ago. He has a family history of migraines in his mother and grandmother. He is currently in the 80th percentile for height and weight. On physical exam his temperature is 99°F (37.2°C), blood pressure is 110/75 mmHg, pulse is 100/min, respirations are 19/min, and pulse oximetry is 99% on room air. He is uncooperative for the rest of the physical exam. During workup, a lesion is found in this patient. Which of the following would most likely be seen during histopathologic analysis?
A 62-year-old man presents to his primary care physician because of abdominal pain that started after he went camping several months ago and drank from a mountain stream. This past year, he also went on a trip around the world, eating local foods at each stop. Furthermore, he has had a history of cholelithiasis and had his gallbladder removed 3 years ago. Otherwise, his medical history is significant for well-controlled hypertension and diabetes. Based on clinical suspicion, an endoscopy and biopsy was performed showing a mix of mononuclear cells and a motile, urease-positive, oxidase-positive, spiral shaped organism. The changes seen on biopsy in this patient most likely predispose him to which of the following pathologies?
Practice by Chapter
Characteristics of benign vs malignant tumors
Practice Questions
Nomenclature of neoplasms
Practice Questions
Carcinogenesis models
Practice Questions
Oncogenes and proto-oncogenes
Practice Questions
Tumor suppressor genes
Practice Questions
DNA repair genes and cancer
Practice Questions
Epigenetic mechanisms in cancer
Practice Questions
Apoptosis and cancer
Practice Questions
Tumor angiogenesis
Practice Questions
Tumor invasion and metastasis
Practice Questions
Carcinogenic agents
Practice Questions
Paraneoplastic syndromes
Practice Questions
Tumor immunology
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app