
Neoplasia — MCQs

On this page
A 32-year-old woman comes to the physician for a routine examination. She has no history of serious medical illness. She appears well. Physical examination shows several hundred pigmented lesions on the back and upper extremities. A photograph of the lesions is shown. The remainder of the examination shows no abnormalities. This patient is at increased risk of developing a tumor with which of the following findings?

A 35-year-old woman comes to the physician because of a 2-month history of vaginal bleeding after intercourse. Menarche occurred at the age of 13 years and menses occur at regular 28-day intervals. Gynecologic examination shows an irregular lesion at the cervical os. Histological evaluation of a cervical biopsy specimen obtained on colposcopy confirms a diagnosis of in-situ cervical cancer. This cancer is most likely derived from which of the following types of cells?
A 32-year-old man presents to the emergency room for a generalized tonic-clonic seizure. After stabilizing the patient, a full radiologic evaluation reveals multiple contrast-enhancing lesions in the brain, lungs, and liver. According to his wife, he lost several pounds in the last few months. The medical history is relevant for cryptorchidism, with abdominal testes that were surgically transferred to the scrotum just before he turned 1-year old. His lab investigation reveals: α-fetoprotein: 9 ng/mL (normal values < 10 ng/mL) Human chorionic gonadotropin: 1,895 IU/L (normal values < 0.5 IU/L) Which of the following microscopic features best describes the lesions seen in this patient's imaging study?
A 65-year-old man presents with complaints of weakness and swollen gums for the past 3 weeks. He also says he cut his finger while cooking, and the bleeding took more than 10 minutes to stop. He has a family history of diabetes mellitus type 2 and prostate cancer. Current medications are multivitamin. His blood pressure is 122/67 mm Hg, the respiratory rate is 13/min, and the temperature is 36.7°C (98.0°F). On physical examination, the patient seems pale and lethargic. On cardiac exam, a pulmonary valve flow murmur is heard. There is significant hepatosplenomegaly present, and several oral mucosal petechiae in the oral cavity are noted. Gum hypertrophy is also present. A peripheral blood smear reveals myeloperoxidase-positive cells and Auer Rods. A bone marrow biopsy shows > 30% of blast cells. Which of the following chromosomal abnormalities is associated with this patient’s most likely diagnosis?
A 60-year-old man presents to your office because he noticed a "weird patch" on the floor of his mouth. He states that he noticed it a few months ago, but did not report it because it did not hurt. However, he is concerned because it has not regressed and seems to have changed in shape. On examination, you notice the patient has poor dentition and he admits to using chewing tobacco daily. The patch on the floor of his mouth is red with irregular borders. Which of the following would be an appropriate way to counsel this patient on his current condition?
A 47-year-old female comes to the emergency department because of increasing back pain for the past 2 weeks. She is unable to perform her daily chores. One month ago, she fell and hurt her back while working outside in the garden. The pain subsided with over-the-counter acetaminophen. She underwent a left mastectomy 1 year ago for breast cancer. She has type 2 diabetes mellitus. Current medications include metformin, sitagliptin, and a multivitamin. She appears uncomfortable. Her temperature is 38.9°C (102.0°F), pulse is 101/min, and blood pressure is 110/80 mm Hg. Examination of the back shows thoracic vertebral tenderness. She has mild stiffness on neck flexion. Muscle strength is decreased in the lower extremities. Deep tendon reflexes are 2+ bilaterally. Sensation to pain, fine touch, temperature, and proprioception is intact. Her hemoglobin concentration is 13.1 g/dL and leukocyte count is 19,300/mm3. Which of the following is the most appropriate next step in management?
A previously healthy 61-year-old man comes to the physician because of a 3-month history of intermittent fever, easy fatiguability, and a 4.4-kg (9.7-lb) weight loss. Physical examination shows conjunctival pallor. The spleen is palpated 5 cm below the left costal margin. Laboratory studies show a leukocyte count of 75,300/mm3 with increased basophils, a platelet count of 455,000/mm3, and a decreased leukocyte alkaline phosphatase score. A peripheral blood smear shows increased numbers of promyelocytes, myelocytes, and metamyelocytes. Which of the following is the most likely diagnosis?
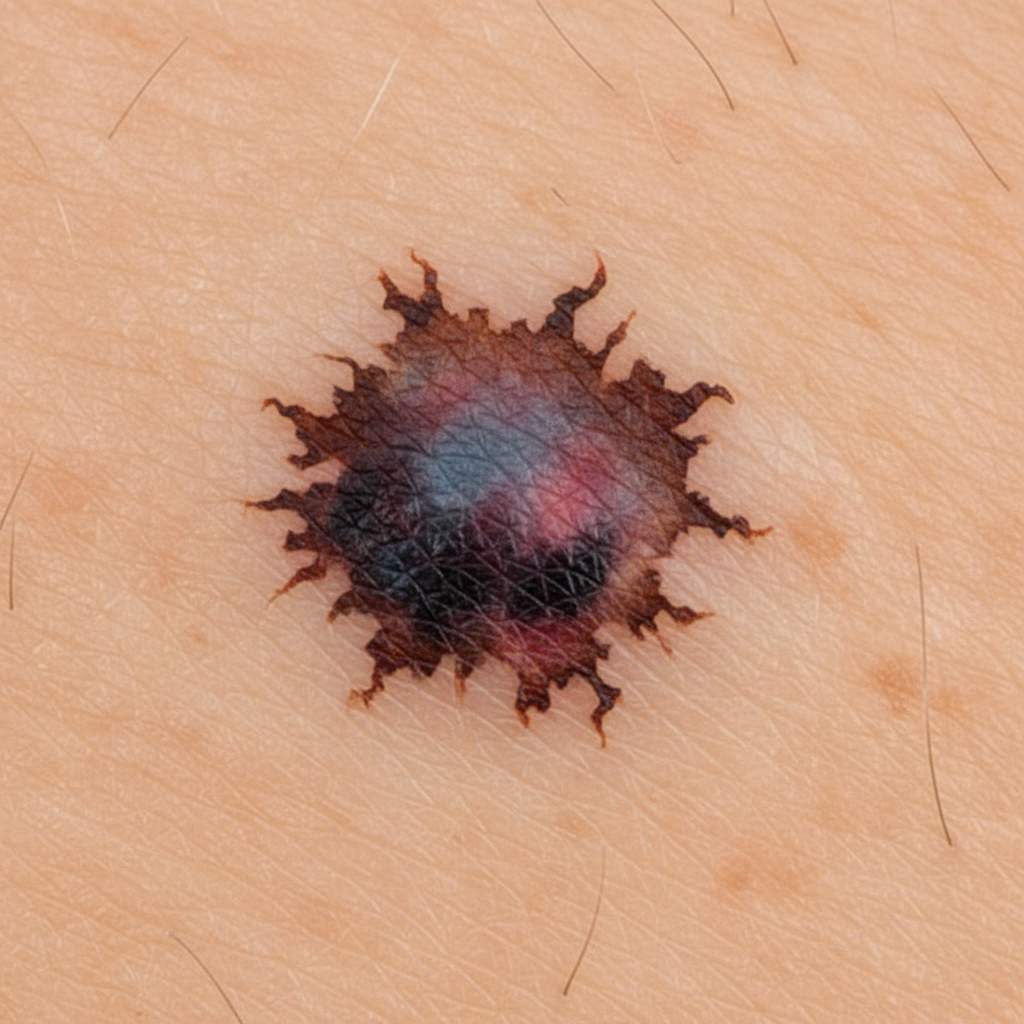
A 52-year-old Caucasian male presents to your office with an 8 mm dark lesion on his back. The lesion, as seen below, has irregular borders and marked internal color variation. Upon excisional biopsy, the presence of which of the following would best estimate the risk of metastasis in this patient's lesion?
A 24-year-old man comes to the physician because of 2 episodes of bleeding from the rectum over the past month. The patient’s father died of colon cancer at the age of 42. The patient has no history of any serious illness and takes no medications. He does not smoke. His vital signs are within normal limits. Physical examination shows a small hard mass over the right mandible that is nontender and fixed to the underlying bone. A similarly hard and painless 5 × 5 mass is palpated over the rectus abdominis muscle. On examination of the rectum, a polypoid mass is palpated at fingertip. Proctosigmoidoscopy shows numerous polyps. Which of the following best explains these findings?
A 53-year-old female visits her physician with watery diarrhea and episodic flushing. The patient reports that she is often short of breath, and a pulmonary exam reveals bilateral wheezing. A CT scan shows a mass in the terminal ileum. 24-hour urine collection shows abnormally elevated 5-hydroxyindoleacetic acid (HIAA) levels. Ultrasound demonstrates a tricuspid valve with signs of fibrosis with a normal mitral valve. A metastatic disease to which organ is most commonly associated with the patient's syndrome?
Practice by Chapter
Characteristics of benign vs malignant tumors
Practice Questions
Nomenclature of neoplasms
Practice Questions
Carcinogenesis models
Practice Questions
Oncogenes and proto-oncogenes
Practice Questions
Tumor suppressor genes
Practice Questions
DNA repair genes and cancer
Practice Questions
Epigenetic mechanisms in cancer
Practice Questions
Apoptosis and cancer
Practice Questions
Tumor angiogenesis
Practice Questions
Tumor invasion and metastasis
Practice Questions
Carcinogenic agents
Practice Questions
Paraneoplastic syndromes
Practice Questions
Tumor immunology
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app