
Neoplasia — MCQs

On this page
A 66-year-old woman presents to the emergency department with abdominal pain. Her symptoms began when she was eating dinner. She has a past medical history of obesity, constipation, intravenous drug use, and diabetes. The patient is instructed to be nil per os and is transferred to the surgical floor. Three days later she had a cholecystectomy and is recovering on the surgical floor. Her laboratory values are ordered as seen below. Hemoglobin: 11 g/dL Hematocrit: 33% Leukocyte count: 8,500/mm^3 with normal differential Platelet count: 197,000/mm^3 Serum: Na+: 139 mEq/L Cl-: 100 mEq/L K+: 4.3 mEq/L HCO3-: 25 mEq/L BUN: 20 mg/dL Glucose: 99 mg/dL Creatinine: 1.1 mg/dL Ca2+: 10.5 mg/dL Alkaline phosphatase: 533 U/L GGT: 50 U/L AST: 22 U/L ALT: 20 U/L The patient is currently asymptomatic and states that she feels well. Which of the following is associated with this patient's underlying condition?
A 56-year-old woman, gravida 3, para 3, comes to the physician because her left breast has become larger, hot, and itchy over the past 2 months. The patient felt a small lump in her left breast 1 year ago but did not seek medical attention at that time. She has hypertension and hyperlipidemia. Menarche was at the age of 11 years and menopause at the age of 46 years. Her mother died of breast cancer at the age of 45 years. The patient does not smoke or drink alcohol. Current medications include labetalol, simvastatin, and daily low-dose aspirin. She is 170 cm (5 ft 7 in) tall and weighs 78 kg (172 lb); BMI is 27 kg/m2. Her temperature is 37.7°C (99.9°F), pulse is 78/min, and blood pressure is 138/88 mm Hg. Examination shows large dense breasts. There is widespread erythema and edematous skin plaques over a breast mass in the left breast. The left breast is tender to touch and left-sided axillary lymphadenopathy is noted. Which of the following is the most likely diagnosis?
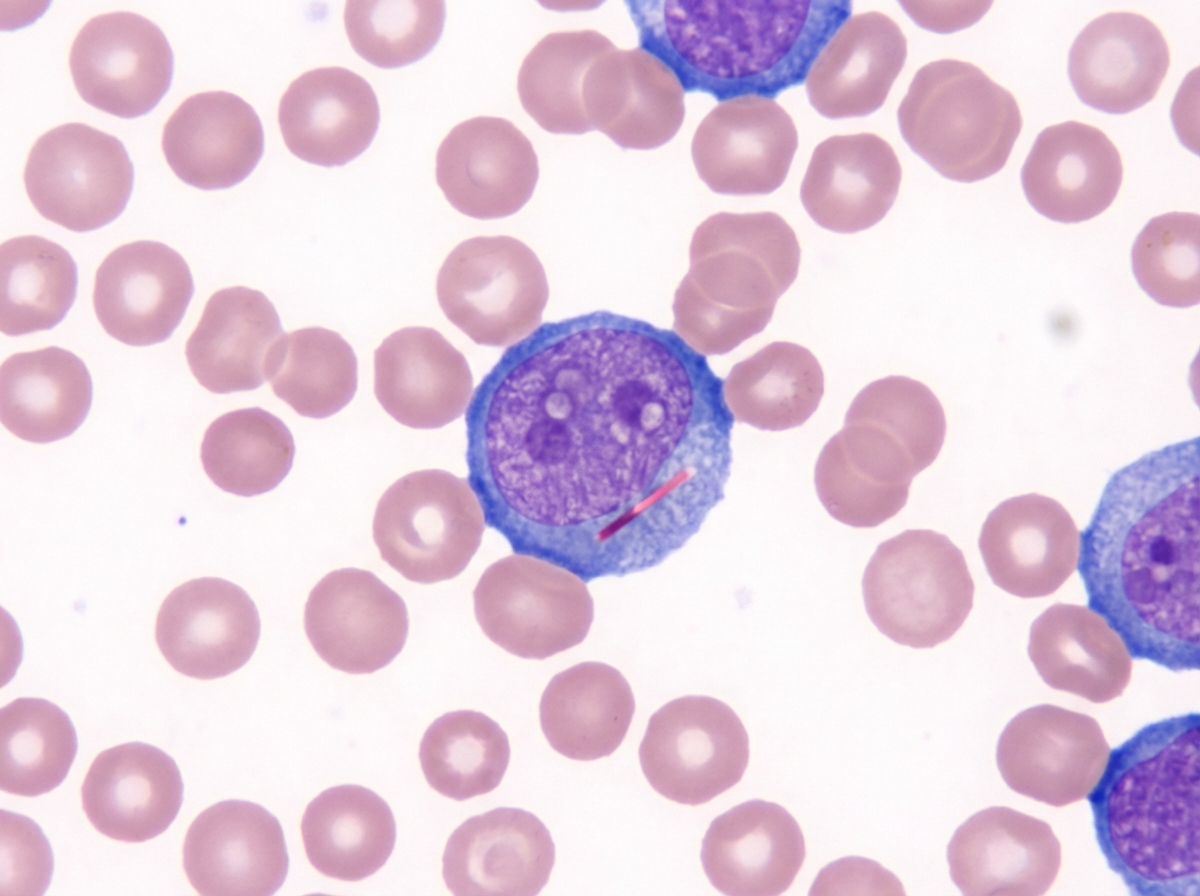
A 63-year-old man presents to the physician with fever for 5 days. He has had increasing fatigue and dyspnea for the past 2 months. During this time, he has lost 3 kg (6.6 lb). He received outpatient treatment for pneumonia last month. He had urinary tract infection 2 weeks ago. He takes no other medications other than daily low dose aspirin and recent oral antibiotics. He does not smoke or drink alcohol. The vital signs include: temperature 38.5°C (101.3°F), pulse 93/min, respiration rate 18/min, and blood pressure 110/65 mm Hg. On physical examination, he has petechiae distally on the lower extremities and several purpura on the trunk and extremities. Several enlarged lymph nodes are detected in the axillary and cervical regions on both sides. The examination of the lungs, heart, and abdomen shows no abnormalities. The laboratory test results are as follows: Hemoglobin 10 g/dL Mean corpuscular volume 90 μm3 Leukocyte count 18,000/mm3 Platelet count 40,000/mm3 A Giemsa-stained peripheral blood smear is shown by the image. Which of the following is the most likely diagnosis?
A 58-year-old lifeguard develops squamous cell carcinoma of the skin on his forehead. Which of the following most likely preceded the development of this carcinoma?
A 40-year-old woman presents to her primary care physician complaining of a several-month history of episodic sweating and heart racing. Her husband noticed that she becomes pale during these episodes. She also has progressive episodic pounding headaches which are not relieved by paracetamol. Her family history is negative for hypertension, endocrinopathies, or tumors. Vital signs reveal a blood pressure of 220/120 mm Hg, temperature (normal) and pulse of 110/min. Fundus examination reveals hypertensive retinal changes. This patient condition is most likely due to neoplasm arising from which of the following?
A 32-year-old G0P0 African American woman presents to the physician with complaints of heavy menstrual bleeding as well as menstrual bleeding in between her periods. She also reports feeling fatigued and having bizarre cravings for ice and chalk. Despite heavy bleeding, she does not report any pain with menstruation. Physical examination is notable for an enlarged, asymmetrical, firm uterus with multiple palpable, non-tender masses. Biopsy confirms the diagnosis of a benign condition. Which of the following histological characteristics would most likely be seen on biopsy in this patient?
A 54-year-old woman comes to the physician because of an ulcer on her left ankle for 6 years. She has had multiple ulcers over her left lower extremity during this period that have subsided with wound care and dressing. She has type 2 diabetes mellitus and gastroesophageal reflux disease. Current medications include metformin, sitagliptin, and omeprazole. She appears anxious. She is 162 cm (5 ft 4 in) tall and weighs 89 kg (196 lb); BMI is 34 kg/m2. Vital signs are within normal limits. Examination shows a 7.5-cm (3-in) ulcer with elevated, indurated margins and a necrotic floor above the left medial malleolus. There are multiple dilated, tortuous veins along the left lower extremity. There is 2+ pretibial edema of the lower extremities bilaterally. The skin around the left ankle appears darker than the right and there are multiple excoriation marks. Cardiopulmonary examination shows no abnormalities. Which of the following is the most appropriate next step in management of this patient's current condition?
A 44-year-old woman presents to the outpatient infectious disease clinic. She has a known history of HIV, well-controlled on HAART for the past 8 years. She currently has no additional significant medical conditions. She feels well and a physical examination is within normal limits. She denies any current tobacco use, alcohol use, or illicit drug use, although she has a history of heroin use (injection). Her vital signs include: temperature, 36.7°C (98.0°F); blood pressure, 126/74 mm Hg; heart rate, 87/min; and respiratory rate, 17/min. She has no complaints and is up to date on all of her vaccinations and preventative care. Which of the following malignancies can be seen and is often associated with AIDS?
A 70-year-old man is at his dermatologist’s office for the treatment of a severely pruritic erythroderma with scaling on his buttocks that has been slowly progressing over the past two weeks. The patient works as a truck driver and has a history of hypertension treated with enalapril. The patient reports having tried an over-the-counter cream on the rash without improvement. The vital signs are within normal range. On physical exam, he has multiple confluent and well-demarcated pink patches on his buttocks and legs with some scaling and enlarged inguinal lymph nodes. The dermatologist orders a skin biopsy that reveals Pautrier microabscesses. What is the most likely diagnosis?
A 37-year-old woman, G1P0, visits her gynecologist's office for a routine prenatal checkup. During her quadruple screening test, her alpha-fetoprotein, β-hCG, and pregnancy-associated plasma protein were all decreased. There is also evidence of increased nuchal translucency on the scanning of the male fetus. A confirmatory test indicates signs of a genetic syndrome. The woman is counseled that her child will most likely have a severe intellectual disability. Physical features of this condition include polydactyly, cleft palate, micrognathia and clenched fists. This genetic condition also affects the formation of the brain and can lead to stillbirth. Most babies do not survive beyond the first year of life. Which of the following is responsible for this type of genetic syndrome?
Practice by Chapter
Characteristics of benign vs malignant tumors
Practice Questions
Nomenclature of neoplasms
Practice Questions
Carcinogenesis models
Practice Questions
Oncogenes and proto-oncogenes
Practice Questions
Tumor suppressor genes
Practice Questions
DNA repair genes and cancer
Practice Questions
Epigenetic mechanisms in cancer
Practice Questions
Apoptosis and cancer
Practice Questions
Tumor angiogenesis
Practice Questions
Tumor invasion and metastasis
Practice Questions
Carcinogenic agents
Practice Questions
Paraneoplastic syndromes
Practice Questions
Tumor immunology
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app