
Neoplasia — MCQs

On this page
A 93-year-old woman is brought to the physician because of a purple area on her right arm that has been growing for one month. She has not had any pain or itching of the area. She has hyperlipidemia, a history of basal cell carcinoma treated with Mohs surgery 2 years ago, and a history of invasive ductal carcinoma of the right breast treated with radical mastectomy 57 years ago. She has had chronic lymphedema of the right upper extremity since the mastectomy. Her only medication is simvastatin. She lives in an assisted living facility. She is content with her living arrangement but feels guilty that she is dependent on others. Vital signs are within normal limits. Physical examination shows extensive edema of the right arm. Skin exam of the proximal upper right extremity shows three coalescing, 0.5–1.0 cm heterogeneous, purple-colored plaques with associated ulceration. Which of the following is the most likely diagnosis?
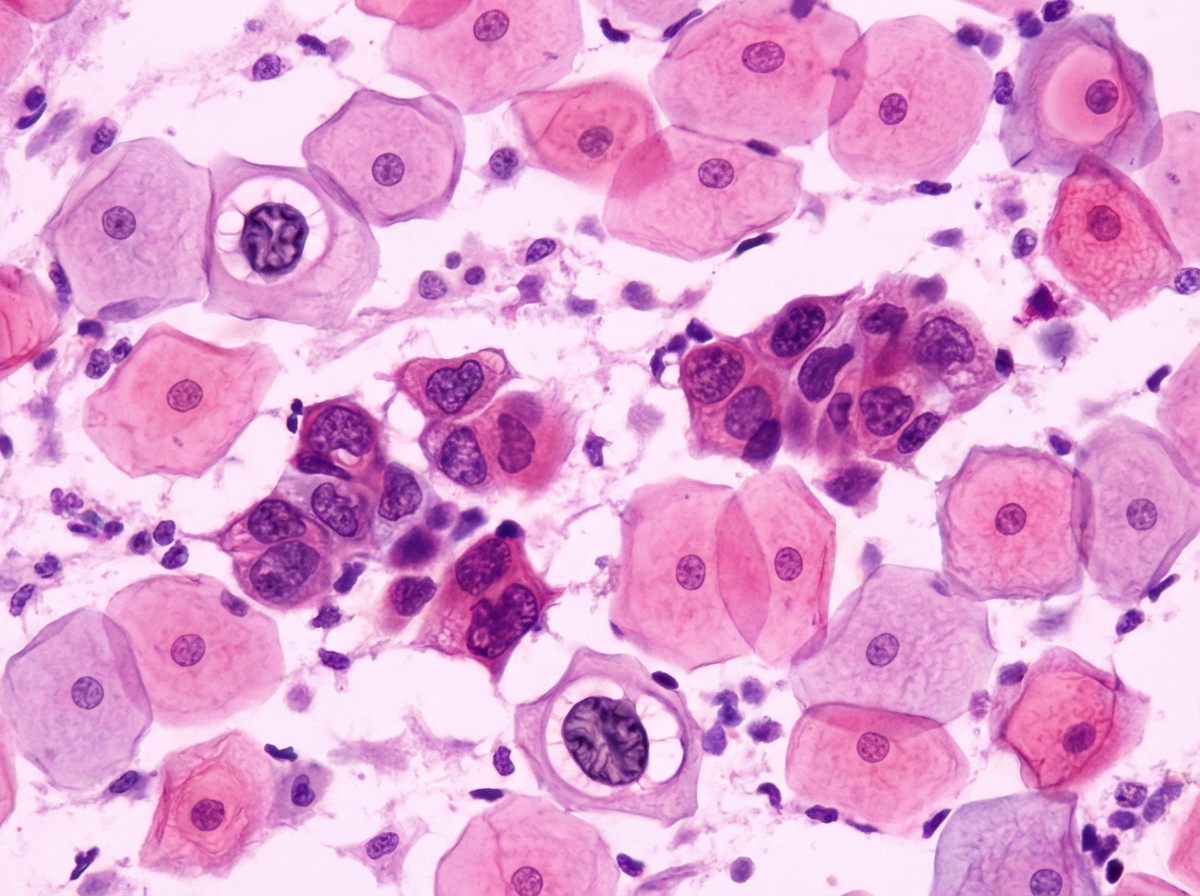
A 41-year-old woman presents with occasional dyspareunia and vaginal bleeding after a sexual encounter. She is in a monogamous relationship and uses oral contraception. She does not have a family history of gynecologic malignancies. She has smoked 1 pack of cigarettes per day for 15 years and drinks several glasses of wine daily. She has not received HPV vaccination. Her blood pressure is 120/70 mm Hg, heart rate is 71/min, respiratory rate is 14/min, and temperature is 36.7°C (98.1°F). A speculum examination shows a nulliparous cervix in the mid-plane of the vaginal vault with a red discoloration—approx. 1 × 2 cm in diameter. Bimanual examination revealed no apparent pathologic changes. A Papanicolaou smear is shown in the exhibit. Which of the following proteins is most likely to be inactivated by viral oncoproteins in the affected cells in this case?
A 53-year-old woman presents to her primary care physician in order to discuss the results of a biopsy. Two weeks ago, her mammogram revealed the presence of suspicious calcifications in her right breast, and she subsequently underwent biopsy of these lesions. Histology of the lesions revealed poorly cohesive cells growing in sheets with a nuclear to cytoplasmic ratio of 1:1. Furthermore, these cells were found to undergo invasion into the surrounding tissues. Given these findings, the patient is referred to an oncologist for further evaluation. Upon further imaging, the patient is found to have no lymph node adenopathy and no distant site metastases. Which of the following would most properly describe the lesions found in this patient?
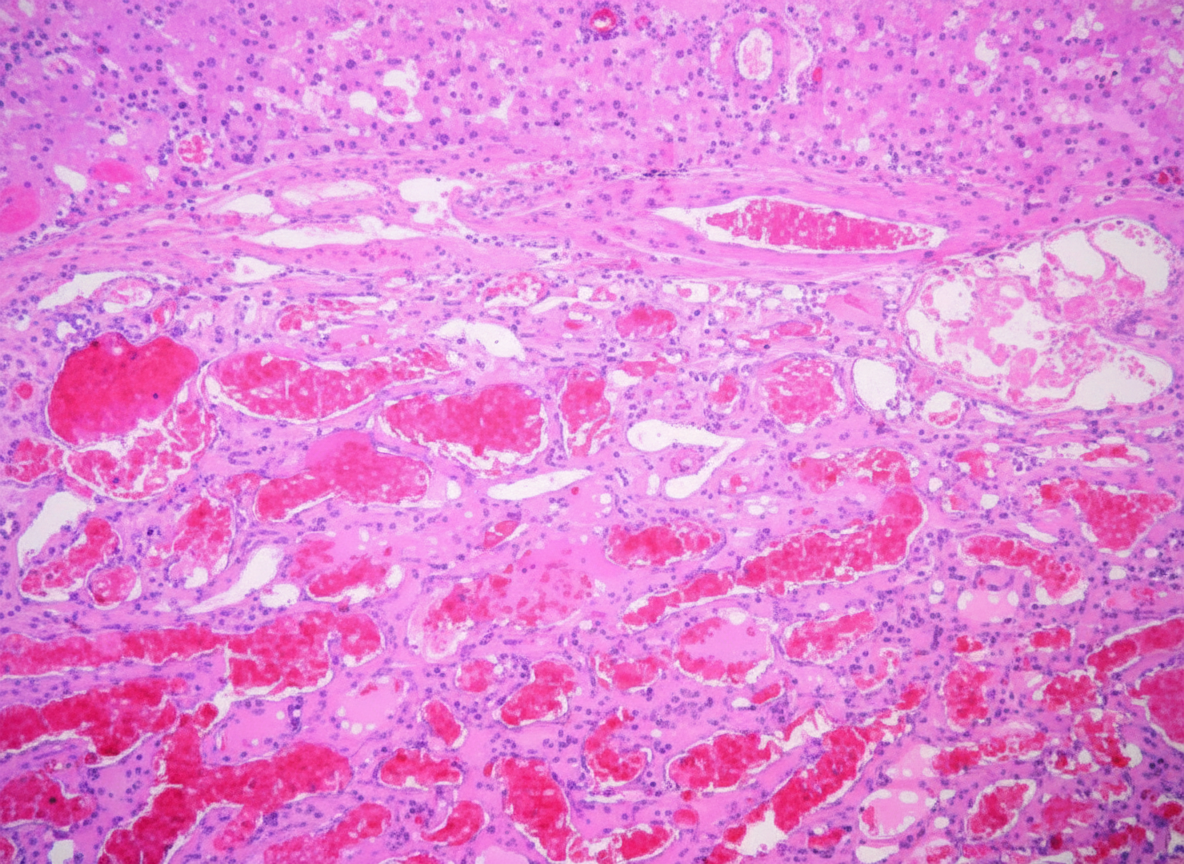
A 49-year-old woman comes to the physician with a 2-month history of mild abdominal pain, nausea, and several episodes of vomiting. She often feels full after eating only a small amount of food. Abdominal examination shows mild right upper quadrant tenderness and a liver span of 16 cm. Ultrasonography shows a 5 x 4 cm hyperechoic mass in the left lobe of the liver. The mass is surgically excised. A photomicrograph of the resected specimen is shown. Which of the following is the most likely diagnosis?
A 74-year-old male presents to his primary care physician complaining of left lower back pain. He reports a four-month history of worsening left flank pain. More recently, he has started to notice that his urine appears brown. His past medical history is notable for gout, hypertension, hyperlipidemia, and myocardial infarction status-post stent placement. He has a 45 pack-year smoking history and drinks 2-3 alcoholic beverages per day. His temperature is 100.9°F (38.3°C), blood pressure is 145/80 mmHg, pulse is 105/min, and respirations are 20/min. Physical examination is notable for left costovertebral angle tenderness. A CT of this patient's abdomen is shown in figure A. This lesion most likely arose from which of the following cells?

A 51-year-old woman presents with the following significant and unintentional weight loss. She denies any personal history of blood clots in her past, but she says that her mother has also had to be treated for pulmonary embolism in the recent past. She also mentions that she had been struggling with her weight, so she was initially content with losing the weight, but her daughter convinced her to come to the office to be checked out. Her past medical history is significant for preeclampsia, hypertension, polycystic ovarian syndrome, and hypercholesterolemia. She currently smokes 1 pack of cigarettes per day, drinks a glass of wine per day, and she currently denies any illicit drug use, although she has a remote past of injection drug use with heroin. The vital signs include: temperature 36.7°C (98.0°F), blood pressure 126/74 mm Hg, heart rate 111/min and irregular, and respiratory rate 17/min. On physical examination, her pulses are bounding and complexion is pale, but breath sounds remain clear. Oxygen saturation was initially 91% on room air and electrocardiogram (ECG) showed atrial fibrillation. Upon further discussion with the patient, her physician discovers that she is having some cognitive difficulty. Her leukocyte count is elevated to 128,000/mm3, and she has elevated lactate dehydrogenase (LDH), uric acid, and B-12 levels. A BCR-ABL translocation is present, as evidenced by the Philadelphia chromosome. What is the most likely diagnosis for this patient?
A 75-year-old man presents to the physician with a complaint of persistent back pain. The patient states that the pain has been constant and occurs throughout the day. He says that he has also been experiencing greater fatigue when carrying out his daily activities. On review of systems, the patient notes that he lost more than 10 pounds in the past month despite maintaining his usual diet and exercising less often due to his fatigue. Physical exam is notable for a systolic murmur at the right sternal border, mild crackles at the bases of both lungs, and tenderness to palpation of his lumbar spine. Laboratory values are below: Serum: Na+: 141 mEq/L Cl-: 101 mEq/L K+: 4.2 mEq/L HCO3-: 23 mEq/L BUN: 20 mg/dL Glucose: 101 mg/dL Creatinine: 1.6 mg/dL Ca2+: 12.8 mg/dL A peripheral blood smear is ordered for the patient’s work-up. Which of the following would be the most likely finding on peripheral blood smear?
A 70-year-old man presents to a medical office with painful micturition for 2 weeks. He denies any other symptoms. The past medical history is unremarkable. He has been a smoker most of his life, smoking approx. 1 pack of cigarettes every day. The physical examination is benign. A urinalysis shows an abundance of red blood cells. A cystoscopy is performed, which reveals a slightly erythematous area measuring 1.5 x 1 cm on the bladder mucosa. A biopsy is obtained and microscopic evaluation shows cells with an increased nuclear: cytoplasmic ratio and marked hyperchromatism involving the full thickness of the epithelium, but above the basement membrane. Which of the following best describes the biopsy findings?
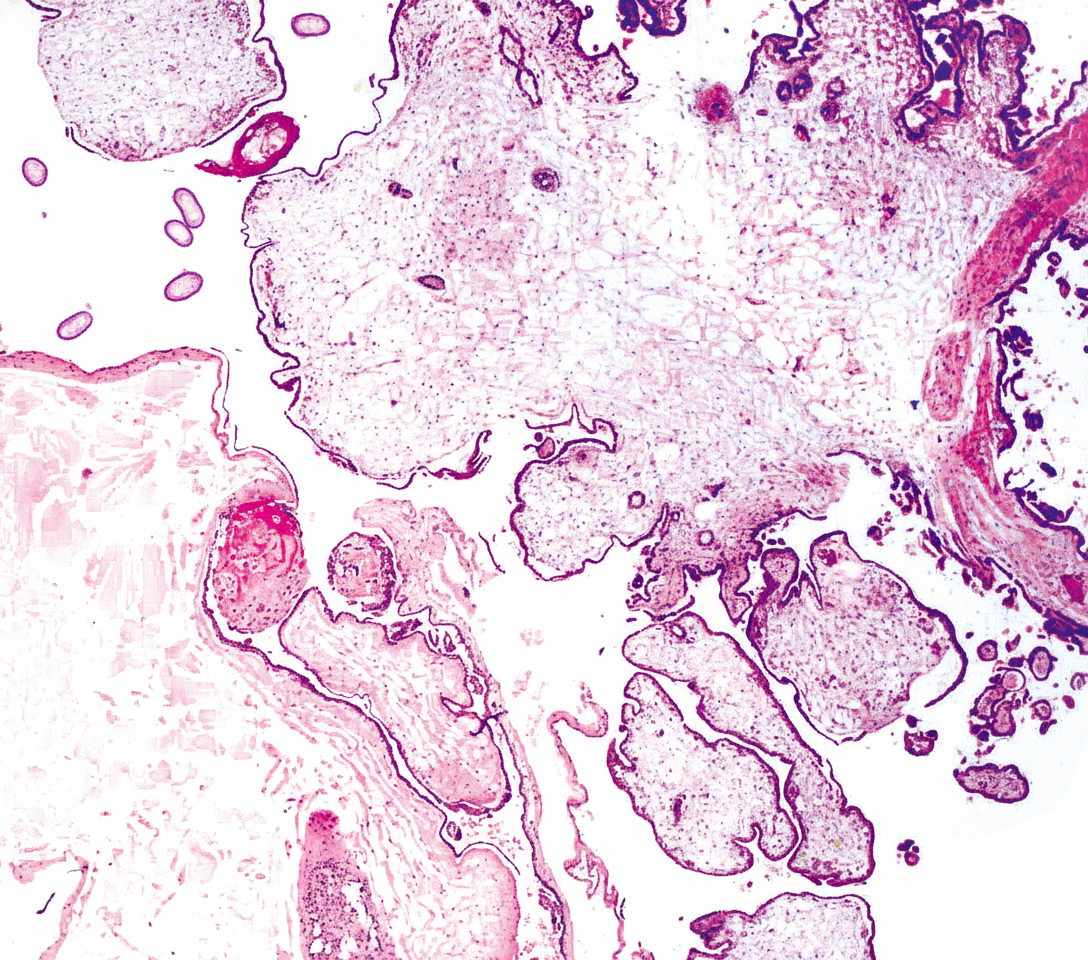
A 29-year-old female reports having a positive home pregnancy test result 9 weeks ago. She presents today with vaginal bleeding and complains of recent onset abdominal pain. Subsequent histologic analysis (Image A) reveals regions of both normal as well as hydropic chorionic villi with focal trophoblastic proliferation. Which of the following is the most likely karyotype associated with this pregnancy?
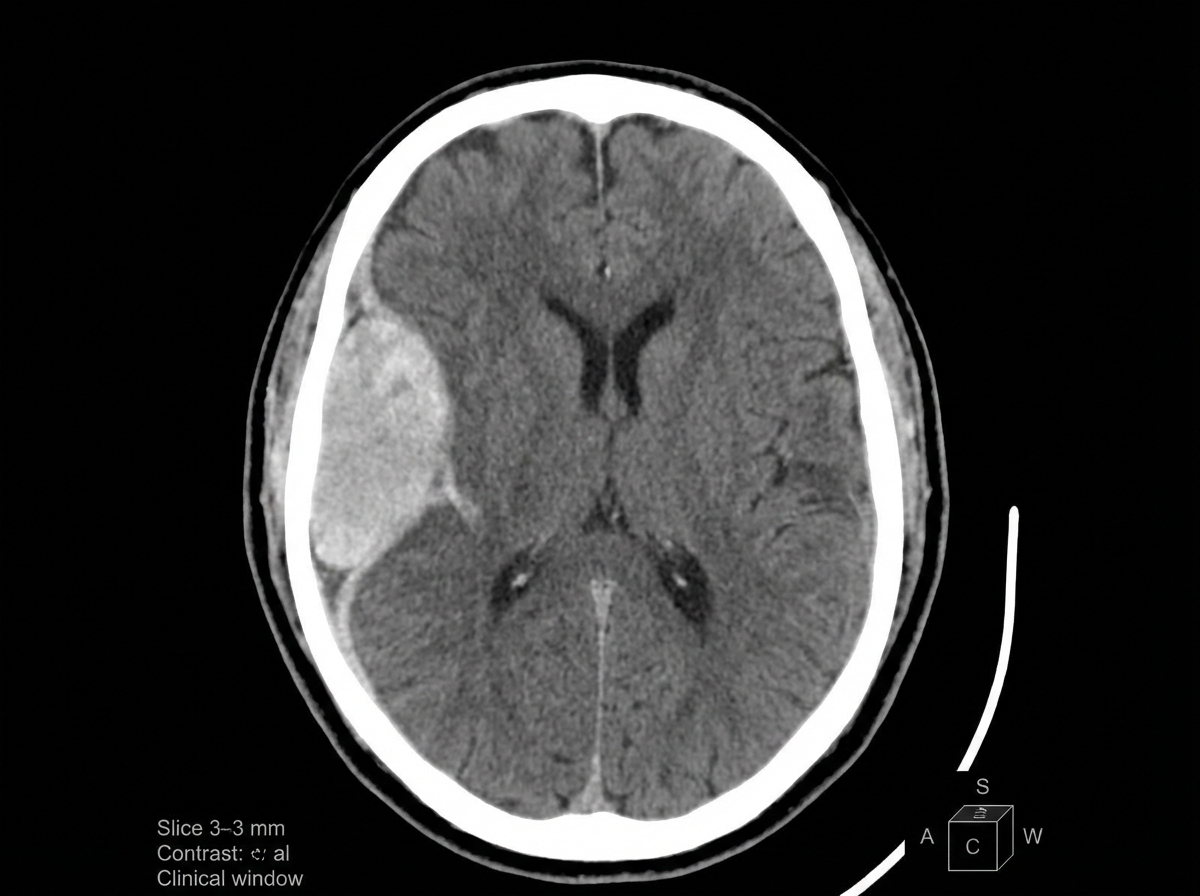
A 41-year-old woman presents to the office with a complaint of a headache for 1 month and an episode of abnormal body movement. The headaches are more severe in the morning, mostly after waking up. She doesn’t give a history of any major illness or trauma in the past. Her vital signs include: blood pressure 160/80 mm Hg, pulse 58/min, temperature 36.5°C (97.8°F), and respiratory rate 11/min. On fundoscopic examination, mild papilledema is present. Her pupils are equal and reactive to light. No focal neurological deficit can be elicited. A contrast computed tomography scan of the head is shown in the picture. Which of the following is the most likely biopsy finding in this case?
Practice by Chapter
Characteristics of benign vs malignant tumors
Practice Questions
Nomenclature of neoplasms
Practice Questions
Carcinogenesis models
Practice Questions
Oncogenes and proto-oncogenes
Practice Questions
Tumor suppressor genes
Practice Questions
DNA repair genes and cancer
Practice Questions
Epigenetic mechanisms in cancer
Practice Questions
Apoptosis and cancer
Practice Questions
Tumor angiogenesis
Practice Questions
Tumor invasion and metastasis
Practice Questions
Carcinogenic agents
Practice Questions
Paraneoplastic syndromes
Practice Questions
Tumor immunology
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app