
Neoplasia — MCQs

On this page
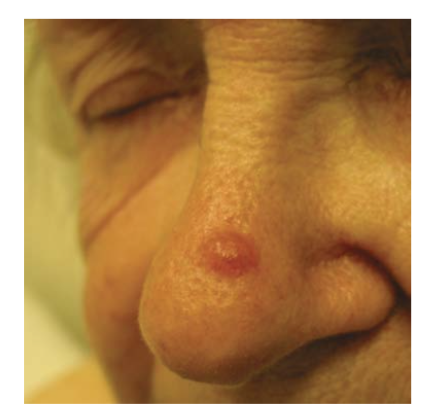
A 62-year-old man comes to the physician because of a skin lesion on his nose. The patient has had the lesion for 11 months and it has increased in size over the past few months. He is a farmer and lives together with his wife. His mother died of metastatic melanoma at the age of 67 years. The patient has smoked a pack of cigarettes daily for the past 30 years and drinks 1–2 glasses of whiskey on weekends. His temperature is 36.8°C (98.2°F), pulse is 75/min, and blood pressure is 140/78 mm Hg. Examination of the skin shows a nontender lesion at the right root of the nose. The lesion is a pearly, translucent papule with a rolled border and visible arborizing telangiectasia on its surface. An image of the lesion is shown. Which of the following is the most likely diagnosis in this patient?
A 50-year-old man presents to his primary care provider complaining of smelling abnormal odors on several occasions. He says that he smells burnt rubber even though there is nothing burning and no one around him can smell what he does. This symptom has been intermittently bothering him for the past 6 months. Also during this period, he had occasional nosebleeds. He works as a high school teacher. Although his work gets a little stressful around the exam season, he says he is able to cope well. Family history is unremarkable. He does not smoke or drink alcohol and denies the use of any medication. Physical examination reveals unilateral nasal obstruction with some dried blood in the nasal passage. What is the most likely diagnosis?
A 57-year-old woman presents to the hospital complaining of 4 months of persistent abdominal pain and early satiety that has recently gotten worse. The patient says that she was prompted to come to the emergency department because she had several episodes of hematemesis. Her last menstrual period was approximately 8 years ago. The patient is sexually active with her husband and notes that she has recently had pain with intercourse as well as 'spotting' after intercourse. The patient states that she has also been experiencing nausea and weight loss associated with abdominal pain. Her blood pressure is 125/84 mm Hg, respiratory rate is 15/min, and heart rate is 76/min. Which of the following would be pathognomonic of this patient’s most likely diagnosis?
A 6-month-old boy is brought to the pediatrician for multiple swellings on his scalp. His mother reports that she first noticed 3 softened and swollen areas over the child's scalp 2 months ago that have grown in size. The child is also urinating more frequently than usual. He was born by cesarean section at 39 weeks gestation. The mother had appropriate prenatal care. She has a history of gastroesophageal reflux disease for which she takes omeprazole. Her family history is unknown as she was adopted at a young age. The boy's temperature is 99°F (37.2°C), blood pressure is 100/60 mmHg, pulse is 110/min, and respirations are 20/min. On exam, he has 3 areas of soft tissue swelling on his skull that are tender to palpation. Moderate asymmetric exophthalmos is noted. A water deprivation test is performed which demonstrates a urine specific gravity of 1.005. The urine specific gravity rises with desmopression administration. A head computerized tomography (CT) scan is performed which demonstrates multifocal lytic calvarial lesions. A biopsy of one of the lesions is performed. Analysis of the biopsy would most likely reveal which of the following findings?
A 46-year-old overweight male presents to his primary care physician for an annual checkup. He has a history of gastroesophageal reflux disease (GERD) with biopsy confirming Barrett's esophagus on therapy with omeprazole. Review of systems is unremarkable, and the patient is otherwise doing well. Vitals are within normal limits and stable. The patient asks about the need for continuing his omeprazole therapy. You recommend he continue his medication because of which of the following most probable long-term sequelae associated with Barrett's esophagus?
A 43-year-old woman presents to a physician with repeated bruising, which she noticed over the last week. Some bruises developed spontaneously, while others were observed following minor trauma. The patient also mentions that she has been experiencing significant fatigue and weakness for the past 4 months and that her appetite has been considerably reduced for a few months. Past medical history is noncontributory. Both of her parents are still alive and healthy. She drinks socially and does not smoke. On physical examination, her temperature is 37.6°C (99.7°F), pulse rate is 88/min, blood pressure is 126/84 mm Hg, and respiratory rate is 18/min. Her general examination reveals mild bilateral cervical and axillary lymphadenopathy with multiple petechiae and ecchymoses over the body. Palpation of the abdomen reveals the presence of hepatomegaly and splenomegaly. Her detailed diagnostic workup, including complete blood counts, coagulation studies, and bone marrow biopsy, confirms the diagnosis of a subtype of acute myeloid leukemia, which is characterized by neoplastic proliferation of promyelocytes and good response to all-trans retinoic acid. The neoplastic cells are myeloperoxidase positive and contain azurophilic crystal rods. Which of the following genetic abnormalities is most likely to be present in this patient?
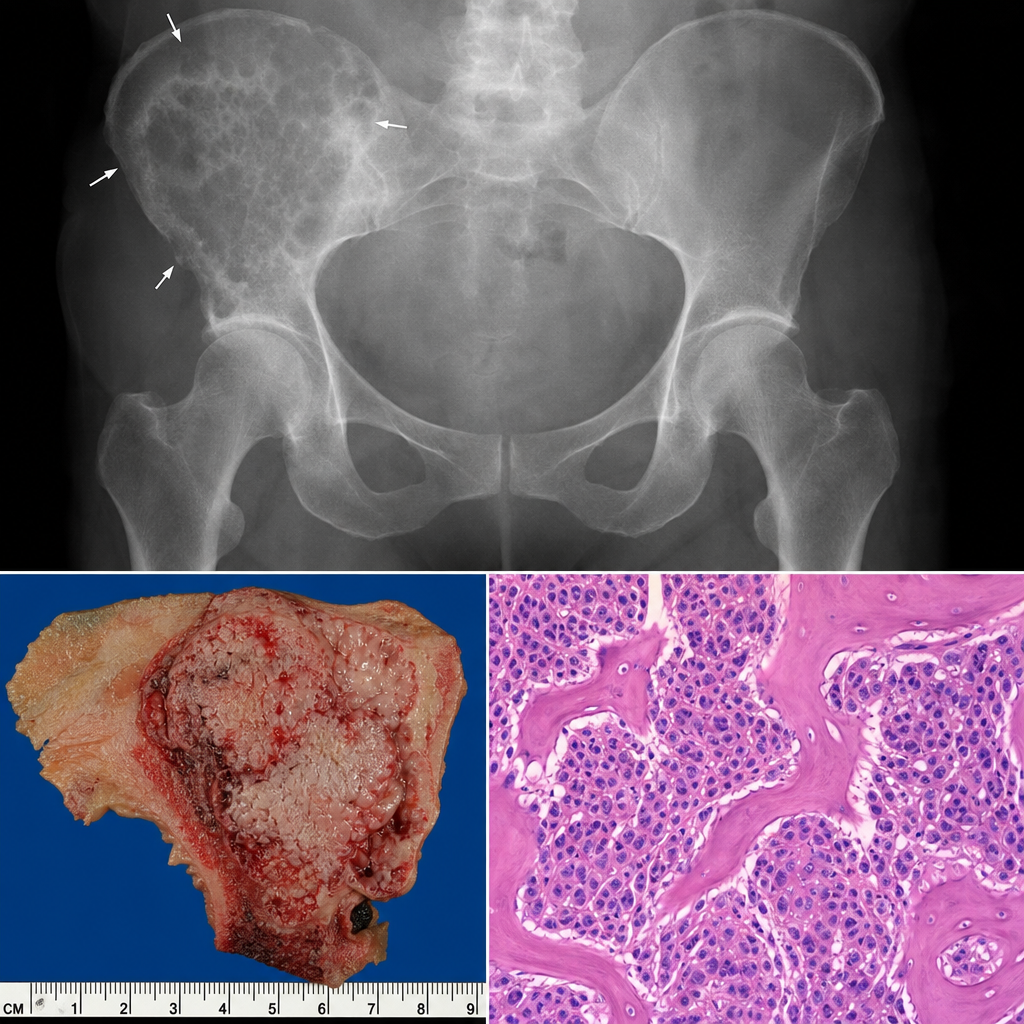
A 69-year-old man comes to the physician because of a 2-month history of severe right hip pain. The pain is worse at night. He has chronic headaches and back pain for which he takes vitamin D, calcium supplements, and ibuprofen. Examination shows hip tenderness and mild sensorineural hearing loss. X-ray of the hip shows a radiolucent lesion in the ilium with a moth-eaten appearance, wide transition zone, and an aggressive periosteal reaction. Wide excision of the lesion is performed. A photomicrograph of a section of the lesion is shown. Which of the following is the most likely diagnosis?
A 68-year-old man comes to the physician 3 months after noticing skin changes on his scalp. When he scrapes off the crust of the lesion, it reappears after a few days. Occasionally, his scalp itches or he notices a burning sensation. He had a mole removed on his right forearm 5 years ago. He is a retired winemaker. His vital signs are within normal limits. Examination shows multiple rough patches on his scalp. A photograph is shown. Which of the following is the most likely diagnosis?

A 38-year-old woman comes to the physician for a 3-month history of bloody discharge from the right nipple. Her mother died of breast cancer at the age of 69 years. Mammography 6 months ago did not show any abnormalities. Examination of the breast shows expression of a small amount of serosanguinous fluid from the right nipple; there are no palpable breast masses or axillary lymphadenopathy. Ultrasonography of the right breast shows a single dilated duct. Which of the following is the most likely diagnosis?
A 68-year-old man comes to the physician because of a several-month history of painless skin lesions on his upper back. The lesions have gradually become darker in color. Sometimes they are itchy. He is a retired gardener. He has smoked half a pack of cigarettes daily for 40 years. His temperature is 36.7°C (98°F), pulse is 72/min, and blood pressure is 123/78 mm Hg. Physical examination shows a cluster of approximately six hyperpigmented plaques on his upper back, the largest measuring approximately 2 cm in diameter, along with several smaller similar lesions, all of which have a greasy and wax-like appearance. A photograph of the upper back is shown. Which of the following is the most likely diagnosis?

Practice by Chapter
Characteristics of benign vs malignant tumors
Practice Questions
Nomenclature of neoplasms
Practice Questions
Carcinogenesis models
Practice Questions
Oncogenes and proto-oncogenes
Practice Questions
Tumor suppressor genes
Practice Questions
DNA repair genes and cancer
Practice Questions
Epigenetic mechanisms in cancer
Practice Questions
Apoptosis and cancer
Practice Questions
Tumor angiogenesis
Practice Questions
Tumor invasion and metastasis
Practice Questions
Carcinogenic agents
Practice Questions
Paraneoplastic syndromes
Practice Questions
Tumor immunology
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app