
Neoplasia — MCQs

On this page
A 73-year-old man is brought to the emergency department because of fever and a productive cough for 2 days. He has had increasing fatigue and dyspnea for the past 2 weeks. During this time he has lost 3 kg (6.6 lb). He received chemotherapy for myelodysplastic syndrome (MDS) 1 year ago. He is currently on supportive treatment and regular blood transfusions. He does not smoke or drink alcohol. The vital signs include: temperature 38.5℃ (101.3℉), pulse 93/min, respiratory rate 18/min, and blood pressure 110/65 mm Hg. He has petechiae distally on the lower extremities and several purpura on the trunk and extremities. Several enlarged lymph nodes are detected in the axillary and cervical regions on both sides. On auscultation of the lungs, crackles are heard in the left lower lobe area. Physical examination of the heart and abdomen shows no abnormalities. The laboratory studies show the following: Hemoglobin 9 g/dL Mean corpuscular volume 95 μm3 Leukocyte count 18,000/mm3 Platelet count 40,000/mm3 Prothrombin time 11 sec (INR = 1) Based on these findings, this patient is most likely to have developed which of the following?
A 34-year-old man comes to the physician because of a 3-week history of left testicular swelling. He has no pain. He underwent a left inguinal hernia repair as a child. He takes no medications. He appears healthy. His vital signs are within normal limits. Examination shows an enlarged, nontender left testicle. When the patient is asked to cough, there is no bulge present in the scrotum. When a light is held behind the scrotum, it does not shine through. There is no inguinal lymphadenopathy. Laboratory studies show: Hemoglobin 14.5 g/dL Leukocyte count 8,800/mm3 Platelet count 345,000/mm3 Serum Glucose 88 mg/dL Creatinine 0.8 mg/dL Total bilirubin 0.7 mg/dL Alkaline phosphatase 35 U/L AST 15 U/L ALT 14 U/L Lactate dehydrogenase 60 U/L β-Human chorionic gonadotropin 80 mIU/mL (N < 5) α-Fetoprotein 6 ng/mL (N < 10) Which of the following is the most likely diagnosis?
A 52-year-old female was found upon mammography to have branching calcifications in the right lower breast. Physical exam revealed a palpable nodularity in the same location. A tissue biopsy was taken from the lesion, and the pathology report diagnosed the lesion as comedocarcinoma. Which of the following histological findings is most likely present in the lesion?
A 43-year-old female presents to her primary care physician complaining of a gradually enlarging neck mass. She reports that she first developed a firm nodular midline mass on the anterior aspect of her neck two months ago. She is otherwise healthy and takes no medications. A fine-needle aspiration is performed and a histological sample of the specimen is shown. Which of the following is the most likely diagnosis?
A 35-year-old man presents to the primary care office with a recent history of frequent falls. He had been able to walk normally until about a year ago when he started noticing that both of his legs felt weak. He's also had some trouble with feeling in his feet. These 2 problems have caused multiple falls over the last year. On physical exam, he has notable leg and foot muscular atrophy and 4/5 strength throughout his bilateral lower extremities. Sensation to light touch and pinprick is absent up to the mid-calf. Ankle jerk reflex is absent bilaterally. His mother mentions that he has always had an unusual foot shape since childhood and that his older brother has similar foot and leg problems. A photo of the patient's foot is shown. Which of the following best describes the etiology of this patient's condition?

A 76-year-old woman is brought to the physician because of lesions on her left arm. She first noticed them 3 months ago and they have grown larger since that time. She has not had any pain or pruritus in the area. She has a history of invasive ductal carcinoma of the left breast, which was treated with mastectomy and radiation therapy 27 years ago. Since that time, she has had lymphedema of the left arm. Physical examination shows extensive edema of the left arm. There are four coalescing, firm, purple-blue nodules on the left lateral axillary region and swelling of the surrounding skin. Which of the following is the most likely diagnosis?
A 12-year-old boy is brought to the emergency department after he vomited and said he was having double vision in school. He also says that he has been experiencing morning headaches, nausea, and dizziness over the last month. He has no past medical history and is not taking any medications. Physical exam reveals a broad-based gait, dysmetria on finger-to-nose testing, and nystagmus. Both serum and urine toxicology are negative, and radiography reveals a solid mass in the midline cerebellum that enhances after contrast administration. Biopsy of this lesion reveals cells of primitive neuroectodermal origin. Which of the following would most likely be seen on histology of this lesion?
A 34-year-old man presents to the office for evaluation of a lesion on his upper arm that appeared a few months ago and has not healed. The patient appears healthful but has a history of cardiovascular disease. He states that his friend at the industrial ammunition factory where he works told him he should "get it looked at." The patient admits to some nausea, vomiting, and diarrhea over the past year, but he states that he "feels fine now." On physical examination, the lesion is an erythematous, scaly, ulcerated plaque on the flexor surface of his upper arm. The rest of the exam is within normal limits. What is the most likely diagnosis?
A 28-year-old man presents with a 3-day history of cough and fever. He says that he recently became a factory worker in a huge plant that is involved in the polyvinyl chloride (PVC) polymerization process. Because he has heard about occupational diseases specifically related to this particular industry, he asks the physician whether his new job is associated with any serious conditions. His physician mentions that polyvinyl chloride is a known chemical carcinogen and that workers who have been exposed to it are known to be at increased risk of developing a particular type of cancer. Which of the following cancers is the physician most likely talking about?
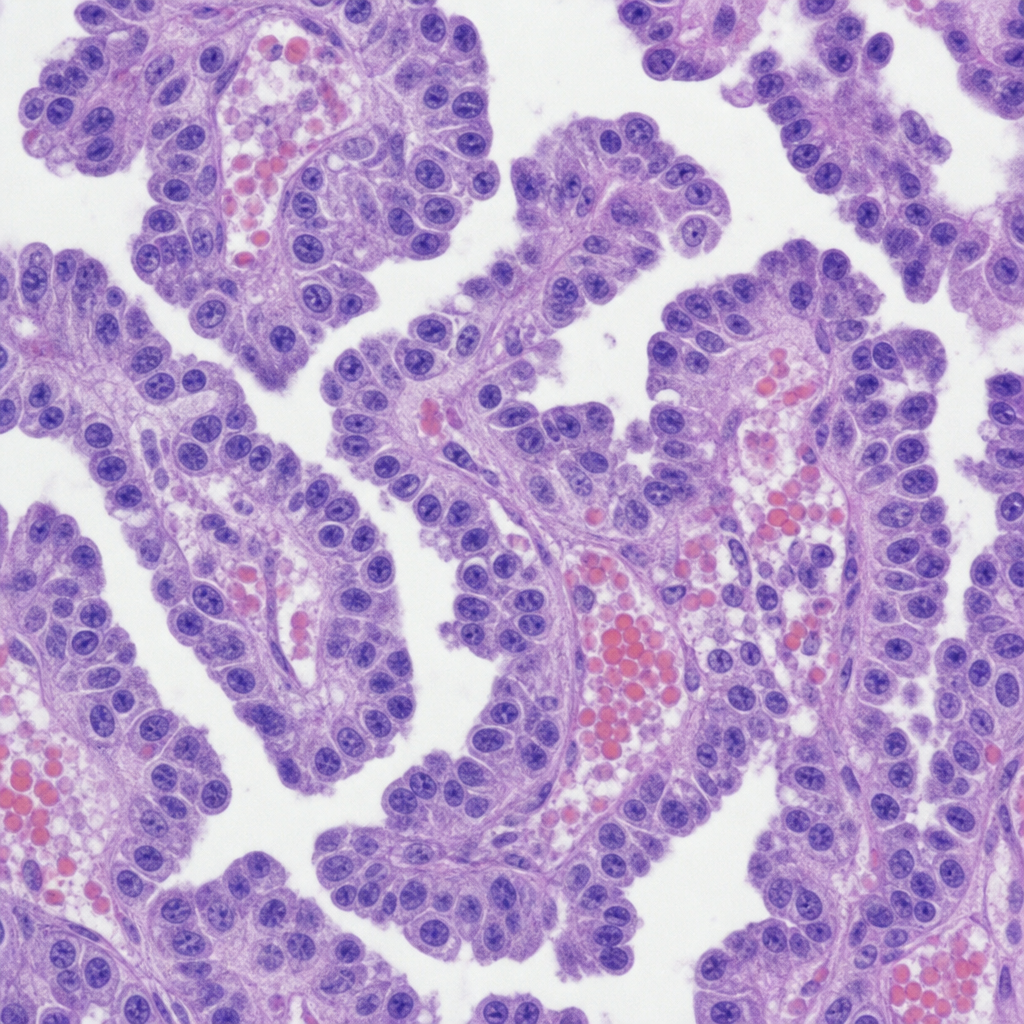
A 47-year-old woman comes to the physician because of a 2-month history of a lump on her neck and a 1-week history of hoarseness. Examination shows a 3-cm, firm, non-tender nodule on the anterior neck. Further evaluation confirms a thyroid malignancy, and she undergoes thyroidectomy. Histopathologic examination of the surgical specimen shows lymphatic invasion. Genetic analysis shows an activating mutation in the RET/PTC genes. Microscopic examination of the surgical specimen is most likely to also show which of the following?
Practice by Chapter
Characteristics of benign vs malignant tumors
Practice Questions
Nomenclature of neoplasms
Practice Questions
Carcinogenesis models
Practice Questions
Oncogenes and proto-oncogenes
Practice Questions
Tumor suppressor genes
Practice Questions
DNA repair genes and cancer
Practice Questions
Epigenetic mechanisms in cancer
Practice Questions
Apoptosis and cancer
Practice Questions
Tumor angiogenesis
Practice Questions
Tumor invasion and metastasis
Practice Questions
Carcinogenic agents
Practice Questions
Paraneoplastic syndromes
Practice Questions
Tumor immunology
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app