
Neoplasia — MCQs

On this page
A 32-year-old man visits his family physician for 10 months of persistent left flank pain, weight loss, and fatigue. Also, he has had hematuria a couple of times in the last month. His mother was diagnosed and treated for a pheochromocytoma when she was 36 years old, and his father died at 45 years due to myocardial infarction. His personal medical history is not relevant. He does not smoke and used to be a varsity athlete in high school and university. Physical examination shows temporal wasting, pale mucous membranes and palms, a palpable mass in the left flank, and a varicocele that does not reduce upon recumbency. His family physician sends the patient to the emergency department for an abdominal computed tomography (CT) scan, which shows a complex left renal mass and a hemangioblastoma in T10. A biopsy of the renal mass is ordered by the oncology team, which demonstrates compact cells with prominent nucleoli, eosinophilic cytoplasm within a network of a small and thin-walled vasculature. What is the most likely type of tumor in this patient?
A 72-year-old male visits his gastroenterologist for a check-up one year following resection of a 2-cm malignant lesion in his sigmoid colon. Serum levels of which of the following can be used in this patient to test for cancer recurrence?
A 15-year-old girl comes to the physician because of a sore throat and subjective fevers for the past 2 weeks. She has been feeling lethargic and is unable to attend school. She has a history of multiple episodes of streptococcal pharyngitis treated with amoxicillin. She immigrated with her family to the United States from China 10 years ago. She appears thin. Her temperature is 37.8°C (100°F), pulse is 97/min, and blood pressure is 90/60 mm Hg. Examination shows pharyngeal erythema and enlarged tonsils with exudates and palatal petechiae. There is cervical lymphadenopathy. The spleen is palpated 2 cm below the left costal margin. Her hemoglobin concentration is 12 g/dL, leukocyte count is 14,100/mm3 with 54% lymphocytes (12% atypical lymphocytes), and platelet count is 280,000/mm3. A heterophile agglutination test is positive. The underlying cause of this patient's symptoms is most likely to increase the risk of which of the following conditions?
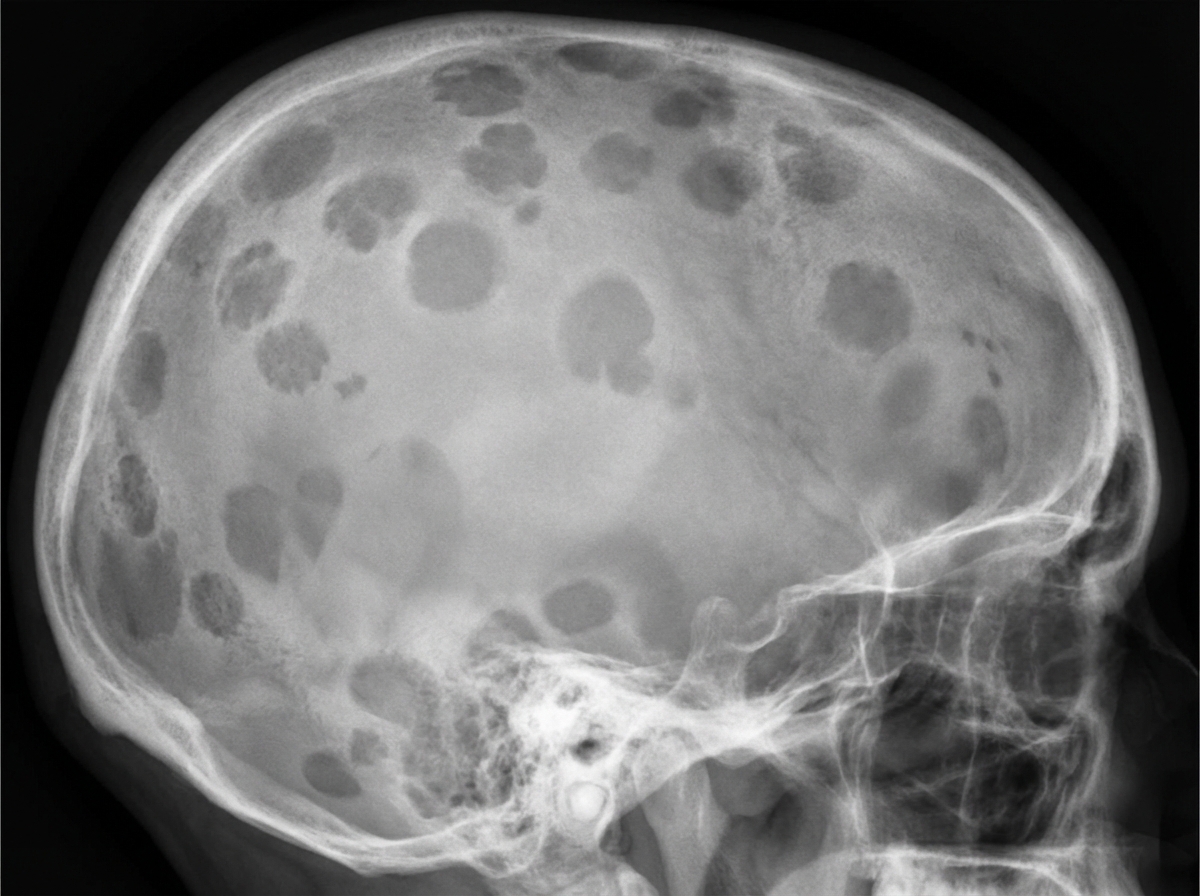
A 70-year-old man comes to the physician because of progressive fatigue and lower back pain for the past 4 months. The back pain worsened significantly after he had a minor fall while doing yard work the previous day. For the past year, he has had a feeling of incomplete emptying of his bladder after voiding. His vital signs are within normal limits. Examination shows bilateral paravertebral muscle spasm, severe tenderness over the second lumbar vertebra, and mild tenderness over the lower thoracic vertebrae. Neurologic examination shows no abnormalities. His hemoglobin is 10.5 g/dl, alkaline phosphatase is 110 U/L, and serum calcium is 11.1 mg/dl. An x-ray of the skull is shown. Which of the following is the most appropriate next step in diagnosis?
A 9-year-old boy is brought to the physician for evaluation of 2 months of progressive clumsiness, falls, and increased urinary frequency. Physical examination shows bilateral temporal visual field loss. An MRI of the head shows a small calcified suprasellar mass. The patient undergoes surgery with complete removal of the mass. Pathological examination of the specimen shows a lobular tumor composed of cysts filled with oily, brownish-yellow fluid. This mass is most likely derived from which of the following structures?
A previously healthy 75-year-old woman comes to the physician because of fatigue and decreasing exercise tolerance over the past 6 weeks. She also has intermittent episodes of dizziness. She has never smoked and does not drink alcohol. She takes a daily multivitamin. She appears pale. Physical examination shows a smooth liver that is palpable 1 cm below the costal margin. The spleen is not palpable. Laboratory studies show: Hemoglobin 9.8 g/dL MCV 104 fL Reticulocyte count 0.2 % Folate 21 ng/mL (N = 2–20) Vitamin B12 789 pg/mL (N = 200–900) A peripheral blood smear shows anisocytosis and bone marrow aspirate shows ringed sideroblasts. This patient is most likely to develop which of the following?
A 52-year-old man is brought to the emergency department because of headaches, vertigo, and changes to his personality for the past few weeks. He was diagnosed with HIV 14 years ago and was started on antiretroviral therapy at that time. Medical records from one month ago indicate that he followed his medication schedule inconsistently. Since then, he has been regularly taking his antiretroviral medications and trimethoprim-sulfamethoxazole. His vital signs are within normal limits. Neurological examination shows ataxia and apathy. Mini-Mental State Examination score is 15/30. Laboratory studies show: Hemoglobin 12.5 g/dL Leukocyte count 8400/mm3 Segmented neutrophils 80% Eosinophils 1% Lymphocytes 17% Monocytes 2% CD4+ T-lymphocytes 90/μL Platelet count 328,000/mm3 An MRI of the brain with contrast shows a solitary ring-enhancing lesion involving the corpus callosum and measuring 4.5 cm in diameter. A lumbar puncture with subsequent cerebrospinal fluid analysis shows slight pleocytosis, and PCR is positive for Epstein-Barr virus DNA. Which of the following is the most likely diagnosis?
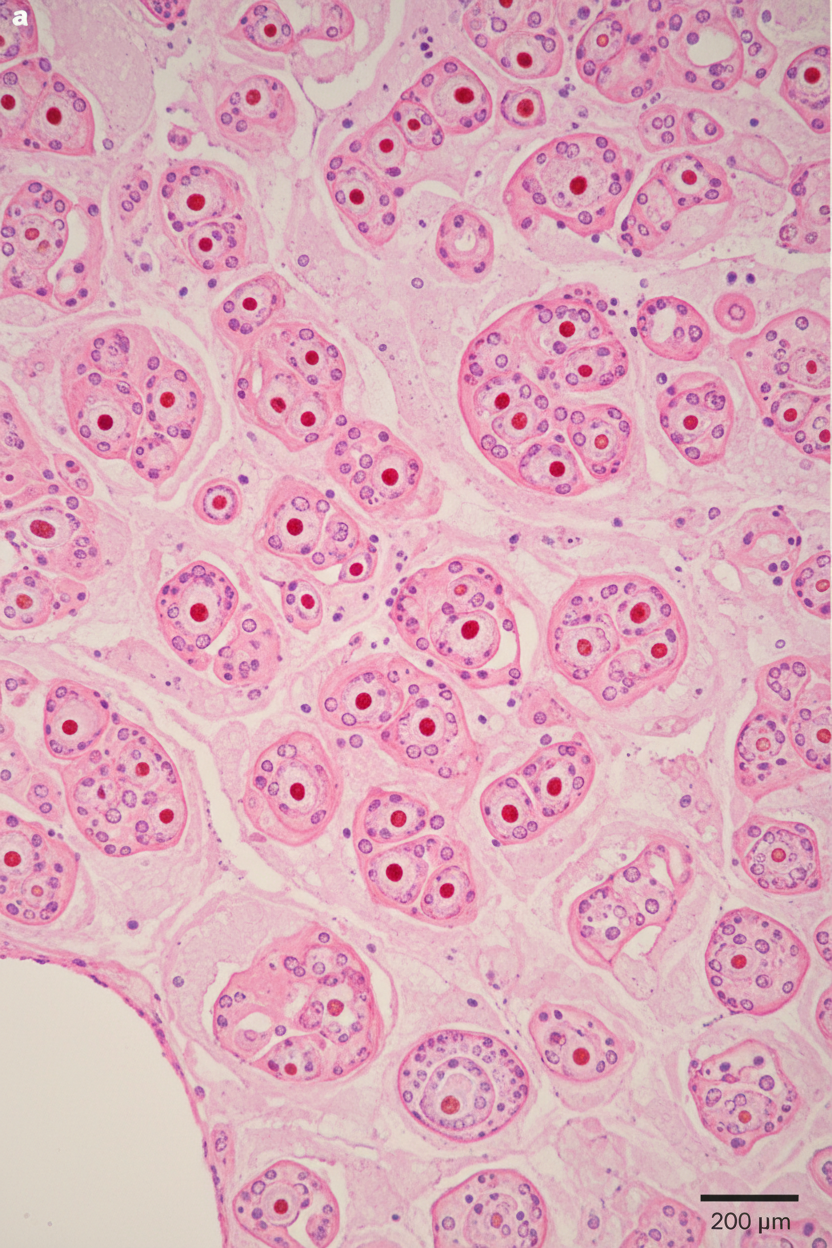
A 57-year-old man comes to the physician with a 3-month history of right flank pain. Urinalysis shows 60 RBC/hpf. Renal ultrasound shows a 3 cm, well-defined mass in the upper pole of the right kidney. A photomicrograph of a section of the resected mass is shown. Which of the following is the most likely diagnosis?
A 67-year-old woman comes to the physician because of a 9-month history of progressive fatigue. Examination shows pallor. Her hemoglobin concentration is 8.9 g/dL, mean corpuscular volume is 75 μm3, and serum ferritin is 9 ng/mL. Test of the stool for occult blood is positive. Colonoscopy shows an irregular, bleeding 3-cm exophytic ulcer in the right colon. Which of the following lesions is the greatest risk factor for this patient's condition?
A 53-year-old woman comes to the emergency department because of blurry vision, headache, and multiple episodes of nosebleeds over the last few weeks. During this time, she has also been itching a lot, especially after getting ready for work in the mornings. She has had an 8-kg (17.6-lb) weight loss and increasing fatigue during the past 6 months. Her temperature is 37.8°C (100.0°F), pulse is 80/min, respirations are 15/min, and blood pressure is 158/90 mm Hg. Physical examination shows no lesions or evidence of trauma in the nasal cavity. Her face, palms, nail beds, oral mucosa, and conjunctiva appear red. Abdominal examination shows splenomegaly. Her hemoglobin concentration is 19 g/dL, hematocrit is 58%, platelets are 450,000/μL, and erythropoietin level is below normal. A peripheral blood smear shows RBC precursor cells. Which of the following is the most likely underlying cause of this patient's condition?
Practice by Chapter
Characteristics of benign vs malignant tumors
Practice Questions
Nomenclature of neoplasms
Practice Questions
Carcinogenesis models
Practice Questions
Oncogenes and proto-oncogenes
Practice Questions
Tumor suppressor genes
Practice Questions
DNA repair genes and cancer
Practice Questions
Epigenetic mechanisms in cancer
Practice Questions
Apoptosis and cancer
Practice Questions
Tumor angiogenesis
Practice Questions
Tumor invasion and metastasis
Practice Questions
Carcinogenic agents
Practice Questions
Paraneoplastic syndromes
Practice Questions
Tumor immunology
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app