
Neoplasia — MCQs

On this page
A 43-year-old man comes to the physician because of weight loss and swelling on the left side of his neck. Physical examination shows a firm, enlarged left upper cervical lymph node that is immobile. Immunohistochemical testing performed on a biopsy specimen from the lymph node stains positive for cytokeratin. Which of the following is the most likely site of the primary neoplasm in this patient?
A 13-year-old boy is brought to the physician because of a 4-month history of worsening dizziness, nausea, and feeling clumsy. An MRI of the brain shows a well-demarcated, 4-cm cystic mass in the posterior fossa. The patient undergoes complete surgical resection of the mass. Pathologic examination of the surgical specimen shows parallel bundles of cells with eosinophilic, corkscrew-like processes. Which of the following is the most likely diagnosis?
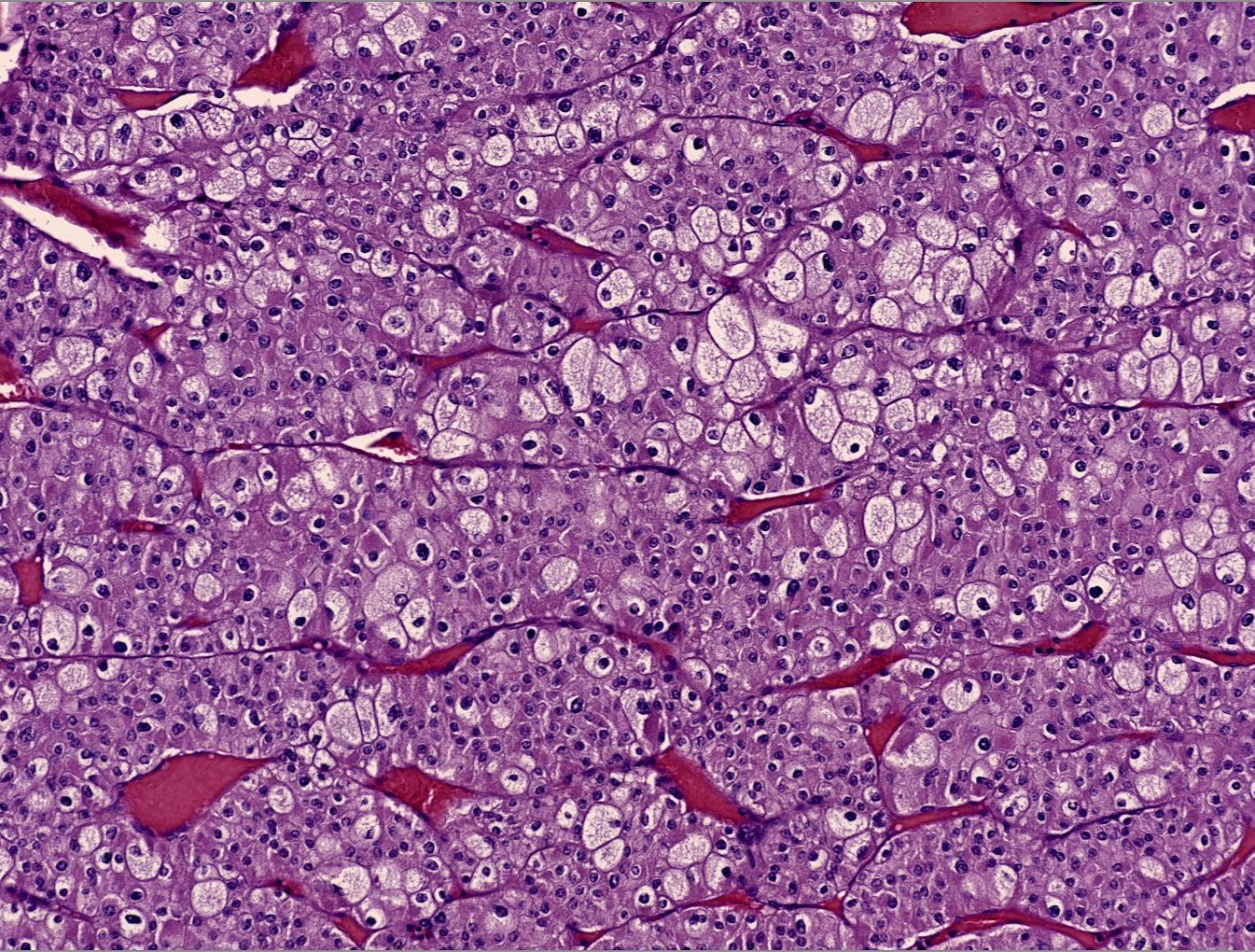
A 69-year-old man comes to the physician because of a 1-week history of blood in the urine and fatigue. He also has had a 5.0-kg (11-lb) weight loss during the past month. Physical examination shows pallor and cachexia. A nontender right flank mass is palpated. A CT scan of the chest, abdomen, and pelvis shows a 5-cm right upper pole renal mass and several pulmonary lesions. A biopsy specimen of an affected area of the lung is obtained. A photomicrograph of the biopsy specimen is shown. Molecular evaluation of the specimen is most likely to show which of the following genetic changes?
A 58-year-old woman with HIV infection is brought to the emergency department because of a 2-week history of headaches, blurred vision, and confusion. Her current medications include antiretroviral therapy and trimethoprim-sulfamethoxazole. Neurological examination shows ataxia and memory impairment. Her CD4+ T-lymphocyte count is 90/μL. Cerebrospinal fluid analysis shows lymphocytic predominant pleocytosis, and PCR is positive for Epstein-Barr virus DNA. An MRI of the brain with contrast shows a solitary, weakly ring-enhancing lesion with well-defined borders involving the corpus callosum. Which of the following is the most likely diagnosis?
An obese 63-year-old man comes to the physician because of 3 episodes of red urine over the past week. He has also had recurrent headaches and intermittent blurry vision during the past month. He has benign prostatic hyperplasia. He works as an attendant at a gas station. The patient has smoked one pack of cigarettes daily for the last 40 years. He does not drink alcohol. Current medications include tamsulosin. His temperature is 37.4°C (99.4°F), pulse is 90/min, and blood pressure is 152/95 mm Hg. Examination shows a flushed face. Cardiopulmonary examination shows no abnormalities. The abdomen is soft and non-tender. Digital rectal examination shows an enlarged prostate with no nodules. Urinalysis shows: Blood 3+ Glucose negative Protein negative WBC 1-2/hpf RBC 40-45/hpf RBC casts none Which of the following is the most likely diagnosis?
A 40-year-old male presents to his primary care physician for a regularly scheduled check-up. Physical examination reveals nontender cervical lymphadenopathy. A biopsy of the lymph node reveals aggregates of follicular architecture, and cytogenic analysis shows a t(14;18) translocation. The protein most likely responsible for the patient’s condition does which of the following:
A 67-year-old man presents to the emergency department with altered mental status. The patient is non-verbal at baseline, but his caretakers at the nursing home noticed he was particularly somnolent recently. The patient has a past medical history of diabetes and Alzheimer dementia. His temperature is 99.7°F (37.6°C), blood pressure is 157/98 mmHg, pulse is 150/min, respirations are 16/min, and oxygen saturation is 98% on room air. Laboratory values are obtained and shown below. Hemoglobin: 9 g/dL Hematocrit: 33% Leukocyte count: 8,500/mm^3 with normal differential Platelet count: 197,000/mm^3 Serum: Na+: 139 mEq/L Cl-: 102 mEq/L K+: 4.3 mEq/L HCO3-: 25 mEq/L BUN: 37 mg/dL Glucose: 99 mg/dL Creatinine: 2.4 mg/dL Ca2+: 12.2 mg/dL The patient has lost 20 pounds over the past month. His parathyroid hormone is within normal limits, and his urinary calcium is increased. Physical exam demonstrates discomfort when the patient's lower back and extremities are palpated. Which of the following is the most accurate diagnostic test for this patient's underlying diagnosis?
A 1-year-old boy is brought to the physician for the evaluation of swelling around the eyelids. He was born at term after an uncomplicated pregnancy. He is at the 95th percentile for weight and 60th percentile for length. His blood pressure is 130/86 mm Hg. Physical examination shows an empty scrotal sac and a left-sided abdominal mass. Ophthalmologic examination shows no abnormalities. Urinalysis shows a proteinuria of 3+ and fatty casts. Abdominal ultrasound shows a hypervascular mass at the upper pole of the kidney. Which of the following best describes the pathogenesis of this patient's disease?
A 6-year-old boy is brought to the physician by his parents because of right lower extremity weakness, worsening headaches, abdominal pain, dark urine, and a 5-kg (11-lb) weight loss for the past 2 months. His teachers report that he has not been paying attention in class and his grades have been worsening. He has a history of infantile seizures. Physical examination shows a palpable abdominal mass and left costovertebral angle tenderness. Neurological exam shows decreased strength of the right lower limb. He has several acne-like angiofibromas around the nose and cheeks. Further evaluation is most likely to show which of the following?
An 11-month-old boy presents with a scaly erythematous rash on his back for the past 2 days. No significant past medical history. Family history is significant for the fact that the patient’s parents are first-degree cousins. In addition, his older sibling had similar symptoms and was diagnosed with a rare unknown skin disorder. On physical examination, whitish granulomatous plaques are present in the oral mucosa, which exhibit a tendency to ulcerate, as well as a scaly erythematous rash on his back. A complete blood count reveals that the patient is anemic. A plain radiograph of the skull shows lytic bone lesions. Which of the following immunohistochemical markers, if positive, would confirm the diagnosis in this patient?
Practice by Chapter
Characteristics of benign vs malignant tumors
Practice Questions
Nomenclature of neoplasms
Practice Questions
Carcinogenesis models
Practice Questions
Oncogenes and proto-oncogenes
Practice Questions
Tumor suppressor genes
Practice Questions
DNA repair genes and cancer
Practice Questions
Epigenetic mechanisms in cancer
Practice Questions
Apoptosis and cancer
Practice Questions
Tumor angiogenesis
Practice Questions
Tumor invasion and metastasis
Practice Questions
Carcinogenic agents
Practice Questions
Paraneoplastic syndromes
Practice Questions
Tumor immunology
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app