
Neoplasia — MCQs

On this page
A 7-year-old boy presents to his primary care physician for a general checkup. The patient has been feeling poorly for the past several weeks and has been losing weight. He states that he often feels weak and too tired to play with his friends. He is no longer interested in many recreational activities he used to be interested in. The patient's parents state that a few of their child's friends have been sick lately. His temperature is 102°F (38.9°C), blood pressure is 77/48 mmHg, pulse is 110/min, respirations are 24/min, and oxygen saturation is 98% on room air. On exam, you note a fatigued appearing child who has lost 10 pounds since his last appointment. Left upper quadrant tenderness and a mass is noted on abdominal exam. Which of the following best describes the most likely diagnosis?
A 25-year-old man presents to his primary care provider complaining of scrotal swelling. He is a college student and plays basketball with his friends regularly. Two days ago, he sustained an injury close to his thigh. He does not have any significant past medical history. Today, his vitals are normal. A focused scrotal examination reveals a firm painless lump on the right testicle which is irregular and small. Ultrasound of the scrotum reveals a vascular 0.6 x 0.5 cm testicular mass. A pelvic lymph node exam is negative. He undergoes a radical orchiectomy and subsequent histopathological examination reveals sheets of small cuboidal cells, multinucleated cells, and large eosinophilic cells with pleomorphic nuclei consistent with choriocarcinoma. Which of the following tumor marker is most likely elevated in this patient?
A 55-year-old woman returns to her physician for a follow-up on the anemia that was detected last month. She received treatment for a nasopharyngeal infection 2 weeks ago. She was diagnosed with small cell lung cancer 2 years ago and was treated with combination chemotherapy. She was a 30-pack-year smoker and quit when she developed lung cancer. She has been a vegan for 2 years. The vital signs are within normal limits. Examination of the lungs, heart, abdomen, and extremities show no abnormalities. No lymphadenopathy is detected. The laboratory studies show the following: Hemoglobin 8.5 g/dL Mean corpuscular volume 105 μm3 Leukocyte count 4,500/mm3 Platelet count 160,000/mm3 An abdominal ultrasonography shows no organomegaly or other pathologic findings. A peripheral blood smear shows large and hypogranular platelets and neutrophils with hypo-segmented or ringed nuclei. No blasts are seen. A bone marrow aspiration shows hypercellularity. In addition, ring sideroblasts, hypogranulation, and hyposegmentation of granulocyte precursors, and megakaryocytes with disorganized nuclei are noted. Marrow myeloblasts are 4% in volume. Which of the following factors in this patient’s history most increased the risk of developing this condition?
A 66-year-old man comes to the physician for a 3-month history of fatigue. He has hypertension and hyperlipidemia. He had a transient ischemic attack 3 years ago. He drinks 3 beers a day, and sometimes a couple more on social occasions. He currently takes aspirin, simvastatin, hydrochlorothiazide, and metoprolol. His temperature is 37.1°C (98.8°F), pulse is 78, respirations are 19/min, and oxygen saturation on room air is 97%. He is in no distress but shows marked pallor and has multiple pinpoint, red, nonblanching spots on his extremities. On palpation, his spleen is significantly enlarged. Laboratory studies show a hemoglobin of 8.0 g/dL, a leukocyte count of 80,000/mm3, and a platelet count of 34,000/mm3. A blood smear shows immature cells with large, prominent nucleoli and pink, elongated, needle-shaped cytoplasmic inclusions. Which of the following is the most likely diagnosis?
A 3-year-old boy is brought to the pediatrician by his parents because of excessive growth and a large tongue. His past medical-social history reveals that he is a product of non-consanguineous marriage to a 20-year-old primigravida. He was born at full term with a birth weight of 3.8 kg (8.4 lb) and length of 52 cm (20.5 in). His temperature is 37.0ºC (98.6°F), pulse is 90/min, and respirations are 22/min. Physical examination shows a mass coming out from his umbilicus and his head circumference is below average compared with children his age. On systemic examination, hepatomegaly is present. Asymptomatic hypoglycemia (36 mg/dL) is also detected, for which dextrose infusion is given. Which of the following is the most likely underlying mechanism that best explains the pathogenesis of this condition?
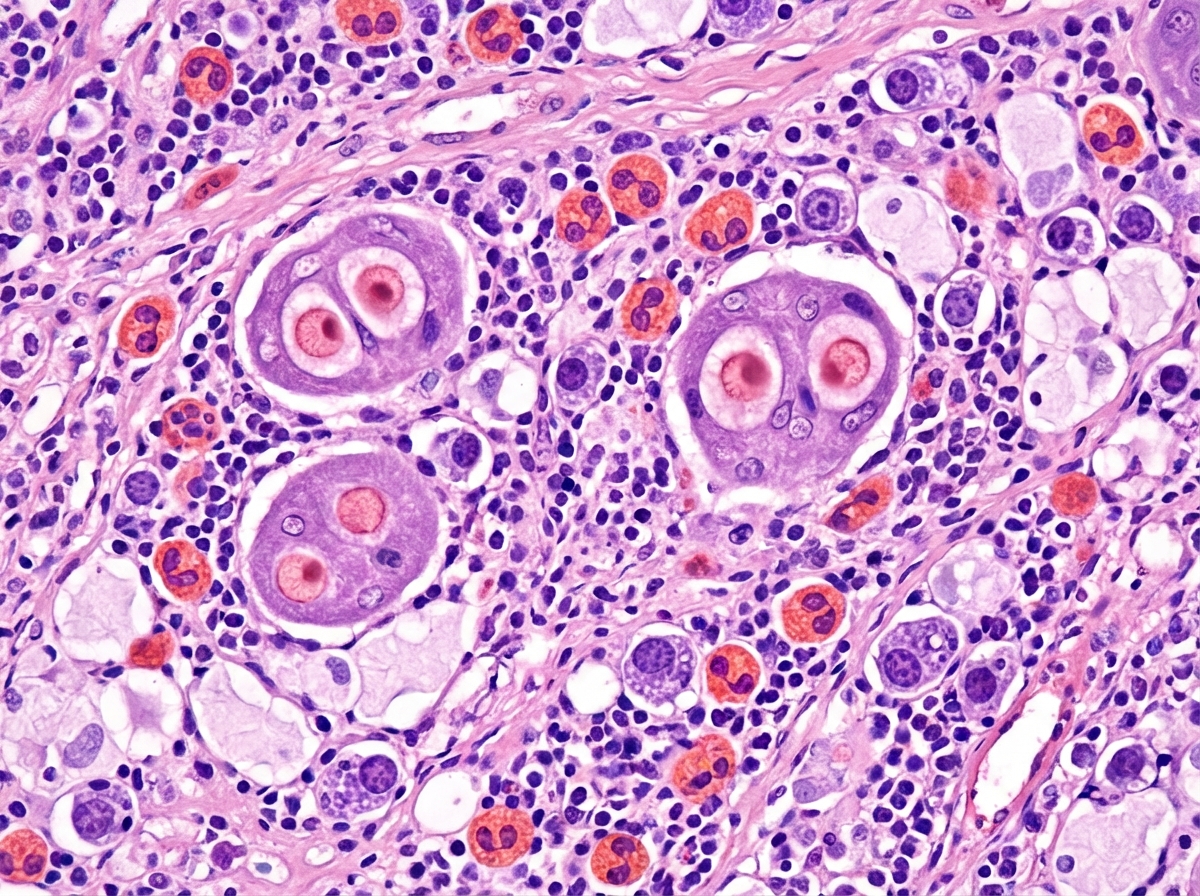
A 58-year-old man presents with a lump on his neck. He says the mass gradually onset 2 months ago and has been progressively enlarging. He denies any pain, weight loss, fevers, chills, or night sweats. Past medical history is significant for HIV, diagnosed 5 years ago, managed on a new HAART regimen he just started. The patient is afebrile and vital signs are within normal limits. Physical examination shows a 3 cm mobile firm mass on the left lateral side of the neck immediately below the level of the thyroid cartilage. A biopsy of the mass is performed and reveals atypical mononuclear cells in a background of eosinophils, plasma cells, histiocytes, atypical T-lymphocytes, and binucleated Reed-Sternberg cells (shown in image). Which of the following is the most likely diagnosis in this patient?
An 82-year-old man presents with painless swelling of the neck for the past week. He reports no recent fever, night sweats, or weight loss. He has no significant medical history, and his only medication is daily aspirin. His temperature is 36.8℃ (98.2℉). On physical examination, there are several non-tender lymph nodes, each averaging 2 cm in diameter, which are palpable in the right anterior cervical triangle. No other palpable lymphadenopathy is noted. The remainder of the physical exam is unremarkable. Laboratory studies show the following: Hemoglobin 10 g/dL Leukocyte count 8000/mm3 with a normal differential Platelet count 250,000/mm3 Erythrocyte sedimentation rate 30 mm/h An excisional biopsy of a cervical lymph node reveals the presence of Reed-Sternberg (RS) cells. Computed tomography (CT) scans and positron emission tomography (PET) scans reveal no mediastinal mass or signs of additional disease. Which of the following aspects most strongly indicates a good prognosis for this patient?
A 69-year-old woman comes to the physician because of lower back pain and right-sided chest pain for the past month. The pain is aggravated by movement. Over the past 2 months, she has had increasing fatigue. Her mother died of breast cancer. She has hypertension and reflux disease. Current medications include metoprolol and omeprazole. Vital signs are within normal limits. Examination shows full muscle strength. There is tenderness to palpation over the lower spine and the right lateral chest. The remainder of the examination shows no abnormalities. Laboratory studies show: Hemoglobin 9.5 g/dL Leukocyte count 7,300/mm3 Platelet count 230,000/mm3 Serum Na+ 137 mEq/L K+ 3.5 mEq/L Creatinine 1.3 mg/dL An ECG shows no evidence of ischemia. An x-ray of the chest shows lytic lesions in 2 ribs. Blood smear shows aggregations of erythrocytes. Protein electrophoresis of the serum with immunofixation shows an M-protein spike. This patient's condition is most likely associated with which of the following findings?
A 63-year-old male is accompanied by his wife to his primary care doctor complaining of shortness of breath. He reports a seven-month history of progressively worsening dyspnea and a dry non-productive cough. He has also lost 15 pounds over the same time despite no change in diet. Additionally, over the past week, his wife has noticed that the patient appears confused and disoriented. His past medical history is notable for stable angina, hypertension, hyperlipidemia, and diabetes mellitus. He currently takes aspirin, metoprolol, lisinopril, atorvastatin, metformin, and glyburide. He has smoked 1 pack of cigarettes per day for 30 years and previously worked as a mechanic at a shipyard. Physical examination reveals no wheezes, rales, or rhonchi with slightly decreased aeration in the left lower lung field. Mucus membranes are moist with normal skin turgor and capillary refill. Laboratory analysis reveals the following: Na 121 mEq/L K 3.4 mEq/L Cl 96 mEq/L HCO3 23 mEq/L Cr 1.1 mg/dl BUN 17 mg/dl A biopsy of the responsible lesions will most likely demonstrate which of the following findings?
A 65-year-old man comes to the physician for a routine health maintenance examination. He has a strong family history of colon cancer. A screening colonoscopy shows a 4 mm polyp in the upper sigmoid colon. Which of the following findings on biopsy is associated with the lowest potential for malignant transformation into colorectal carcinoma?
Practice by Chapter
Characteristics of benign vs malignant tumors
Practice Questions
Nomenclature of neoplasms
Practice Questions
Carcinogenesis models
Practice Questions
Oncogenes and proto-oncogenes
Practice Questions
Tumor suppressor genes
Practice Questions
DNA repair genes and cancer
Practice Questions
Epigenetic mechanisms in cancer
Practice Questions
Apoptosis and cancer
Practice Questions
Tumor angiogenesis
Practice Questions
Tumor invasion and metastasis
Practice Questions
Carcinogenic agents
Practice Questions
Paraneoplastic syndromes
Practice Questions
Tumor immunology
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app