
Neoplasia — MCQs

On this page
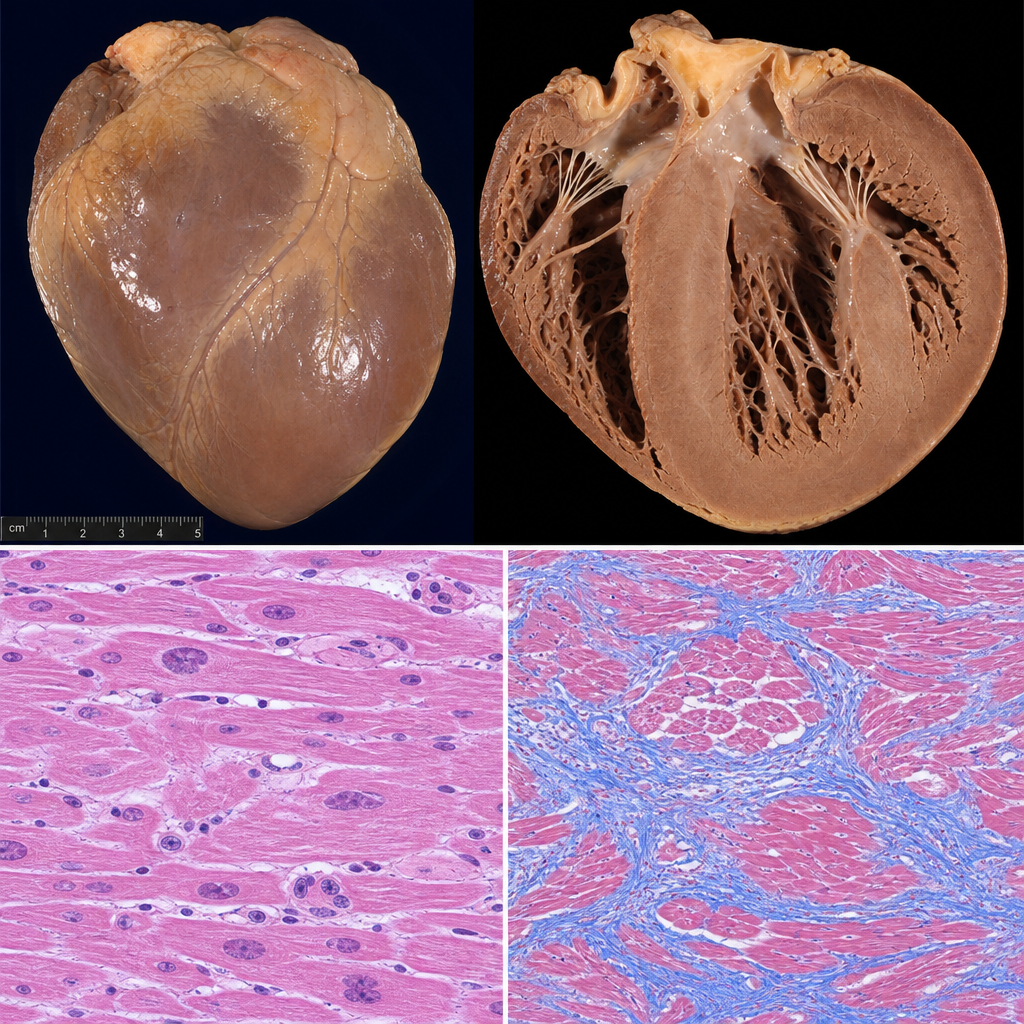
A 62-year-old man with a history of chronic alcohol use dies suddenly. At autopsy, the heart weighs 520 g (normal <400 g) and appears dilated with a flabby myocardium. Histological sections of the myocardium show hypertrophied cardiomyocytes with enlarged, irregular nuclei, and prominent interstitial fibrosis. There is no significant vacuolization of cardiomyocytes. Which of the following best describes the primary histopathologic mechanism underlying the cardiac enlargement and dysfunction in this condition?
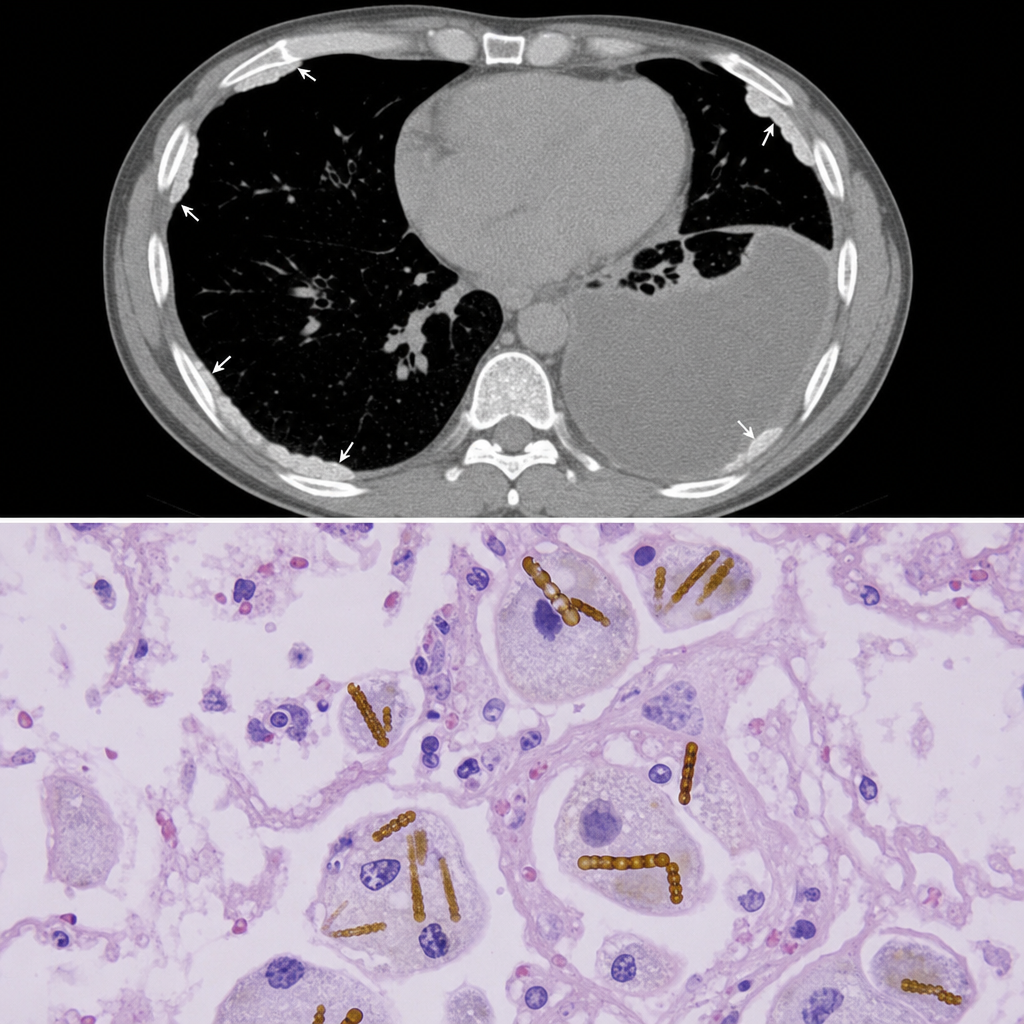
A 58-year-old man with a 40-pack-year smoking history presents with progressive dyspnea and a dry cough. Chest CT reveals bilateral pleural plaques and a right pleural effusion. A transbronchial lung biopsy is performed. The photomicrograph shows elongated, golden-brown, beaded structures with a translucent core surrounded by an iron-protein coat within macrophages and lung parenchyma. Which of the following best describes the pathological significance of this finding?
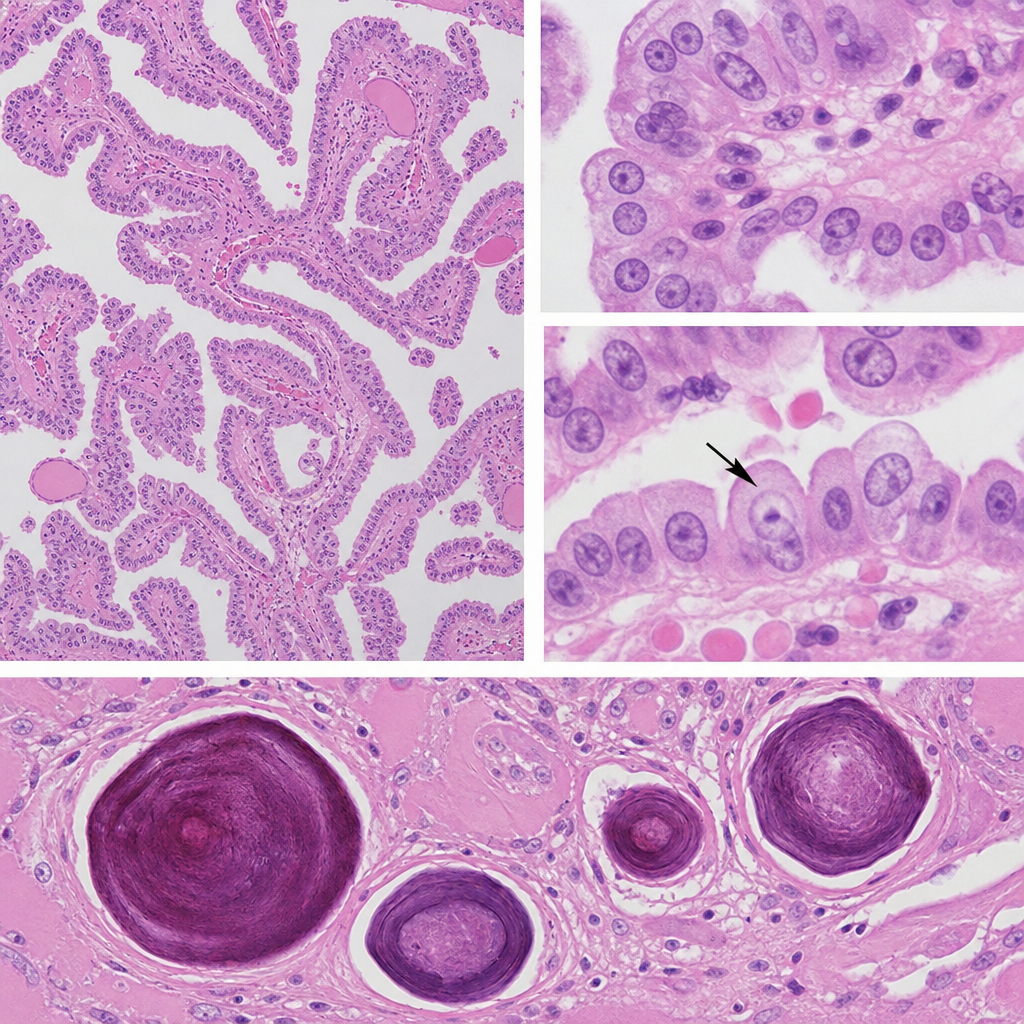
A 52-year-old woman with no significant past medical history undergoes resection of a 2.1 cm thyroid nodule discovered incidentally on ultrasound. Gross examination reveals a lesion with a pale, fleshy cut surface. Histology shows papillary architecture with cells exhibiting ground-glass 'Orphan Annie eye' nuclei, nuclear grooves, and intranuclear cytoplasmic pseudoinclusions. Concentric laminated calcified structures approximately 50–100 µm in diameter are identified within several papillary fronds. The tumor cells are positive for CK19, HBME-1, and galectin-3. Which of the following structures are represented by the concentric calcified findings in this specimen?
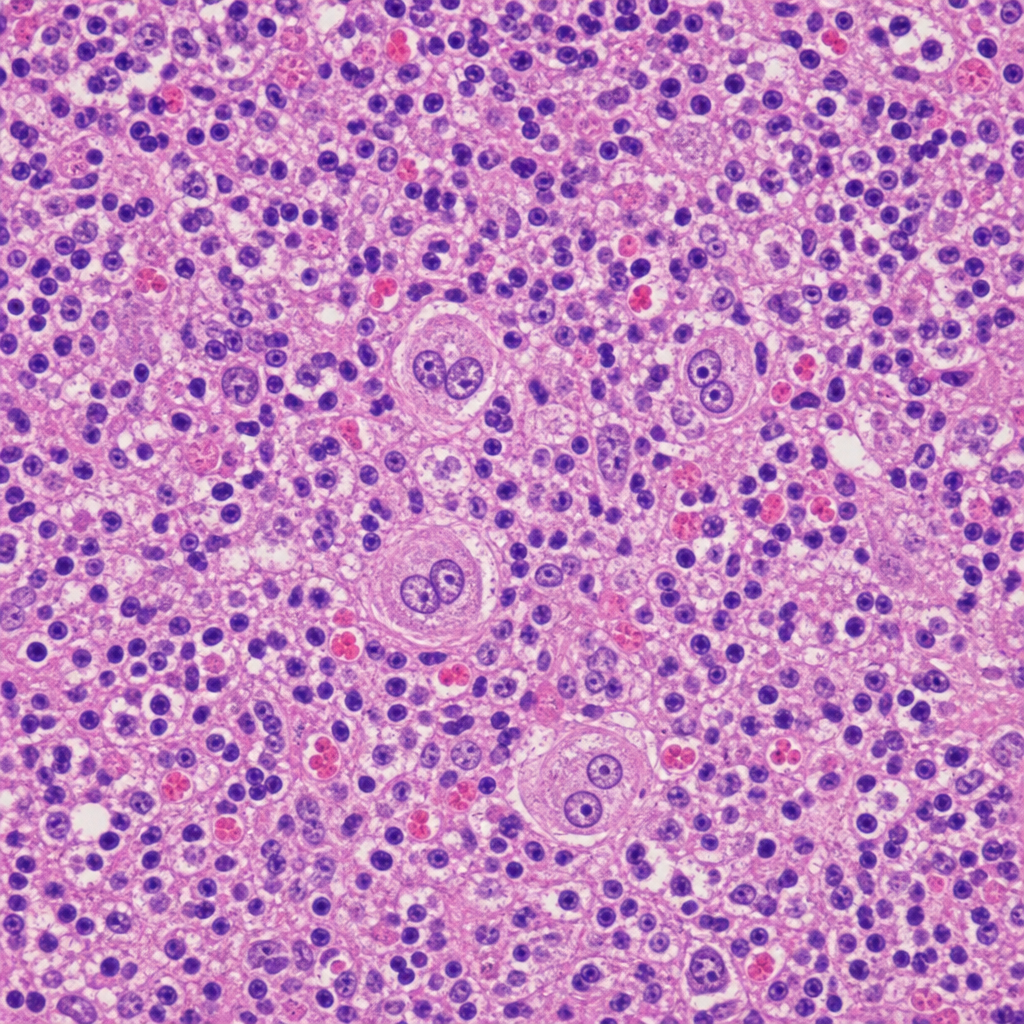
A 34-year-old woman undergoes excisional biopsy of a right axillary lymph node that has been enlarged for 3 months. She reports intermittent fevers, night sweats, and a 6 kg weight loss. The photomicrograph shows effacement of normal nodal architecture by a mixed infiltrate of lymphocytes, eosinophils, plasma cells, and neutrophils. Large binucleate cells with prominent eosinophilic 'owl-eye' nucleoli are present and stain positive for CD15 and CD30 but negative for CD45. A smaller mononuclear variant of the same cell is also visible. Which of the following background inflammatory cell patterns, if identified as predominant on this biopsy, is characteristic of the subtype associated with the worst overall prognosis?
A 61-year-old Caucasian male presents to your office complaining of morning headaches of 6 weeks duration. A head MRI reveals a likely metastasis of unknown origin in the supratentorial region of the brain. On biopsy, the neoplastic mass is shown to have a mutation in BRAF, a protein kinase, in which a glutamic acid is substituted for valine at position 600 of the protein. Where did this metastasis most likely originate?
A 31-year-old woman comes to the emergency department because of a 4-week history of worsening headache, nausea, and vomiting. The headache is worse at night. Fundoscopic examination shows swelling of the optic discs. A CT scan of the brain shows a heterogeneous, hyperintense, intraventricular mass. The patient undergoes surgical excision of the mass. Pathologic examination of the surgical specimen confirms that the tumor is of neuronal origin. The cells in this specimen are most likely to stain positive for which of the following immunohistochemical markers?
A 67-year-old man comes to the physician because of a 4-month history of fatigue and weight loss. Physical examination shows jaundice. The liver is palpated 3 cm below the right costal margin. Serum studies show an elevated alpha-fetoprotein and a prolonged prothrombin time. Genetic analysis of a liver biopsy specimen shows a G:C to T:A transversion in codon 249 of the gene coding for the TP53 protein in affected cells. Which of the following risk factors is most specific to the patient's condition?
A 41-year-old construction worker presents to the office complaining of a progressively worsening breathlessness for the last 2 months. He has no other complaints. His medical history is significant for hypertension being treated with lisinopril-hydrochlorothiazide and gastroesophageal reflux disease being treated with pantoprazole. He has a 30-pack-year smoking history and drinks alcohol on the weekends. He works mainly with insulation and drywall placing. His temperature is 37.0°C (98.6°F), the blood pressure is 144/78 mm Hg, the pulse is 72/min, and the respirations are 10/min. Upon further questioning about his employment, the patient admits that he does not regularly use a mask or other protective devices at work. Which of the following malignancies is this patient most likely at risk for?
A 58-year-old woman with a history of breast cancer, coronary artery disease, gastroesophageal reflux, and diabetes mellitus is diagnosed with angiosarcoma. Which of the following most likely predisposed her to this condition?
A 56-year-old man presents to his primary care physician complaining of a dark spot on his left thigh. He says that he first noticed the spot about 3 years ago when he went to the beach with his family; however, at the time it was very small and he didn't think that it was worth mentioning. Since then, it has been growing slowly and he is now concerned about its size. He says that he does not have any other symptoms associated with the lesion. Physical exam reveals an asymmetric 2.5 centimeter plaque with irregular borders and a varying pattern of brown coloration. The lesion is studied and found to have a mutation in a tumor suppressor gene that normally prevents uncontrolled cell cycle progression by inhibiting cyclin-CDK complexes. Which of the following is most likely true of this gene?
Practice by Chapter
Characteristics of benign vs malignant tumors
Practice Questions
Nomenclature of neoplasms
Practice Questions
Carcinogenesis models
Practice Questions
Oncogenes and proto-oncogenes
Practice Questions
Tumor suppressor genes
Practice Questions
DNA repair genes and cancer
Practice Questions
Epigenetic mechanisms in cancer
Practice Questions
Apoptosis and cancer
Practice Questions
Tumor angiogenesis
Practice Questions
Tumor invasion and metastasis
Practice Questions
Carcinogenic agents
Practice Questions
Paraneoplastic syndromes
Practice Questions
Tumor immunology
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app