
Inflammation — MCQs

On this page
A 12-month-old boy is brought to the physician by his parents for a 4-week history of fever, malaise, cough, and difficulty breathing. He has had recurrent episodes of gastroenteritis since birth. Cardiopulmonary examination shows subcostal retractions and crackles bilaterally. There is enlargement of the cervical, axillary, and inguinal lymph nodes. An x-ray of the chest shows bilateral consolidations. A sputum culture shows colonies of Burkholderia cepacia. A blood sample is obtained and after the addition of nitroblue tetrazolium to the sample, neutrophils remain colorless. A defect in which of the following is the most likely cause of this patient's condition?
A 33-year-old woman comes to the physician because of a 4-day history of fever, anterior neck pain, and throat swelling. She has no history of serious illness. Her temperature is 38.1°C (100.6°F) and pulse is 109/min. Physical examination shows diaphoresis and a fine tremor of the outstretched hands. The thyroid gland is enlarged, firm, and tender to palpation. Serum thyroid stimulating hormone level is 0.06 μU/mL and erythrocyte sedimentation rate is 65 mm/h. 123I scan shows an enlarged thyroid gland with diffusely decreased uptake. Histologic examination of a thyroid biopsy specimen is most likely to show which of the following findings?
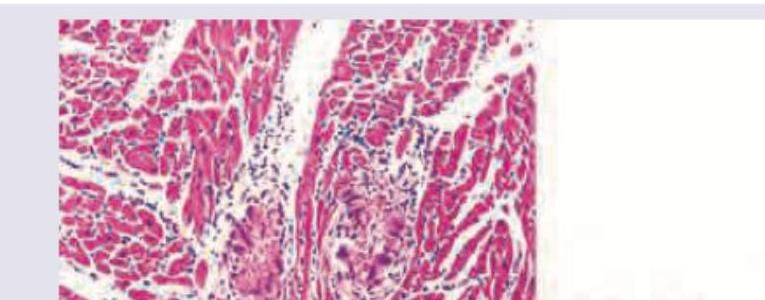
A 9-year-old boy from Eritrea is admitted to the hospital for lethargy and increased work of breathing. He has had recurrent episodes of fever, shortness of breath, and fatigue in the past 3 years. His pulse is 132/min and blood pressure is 90/66 mm Hg. Pulse oximetry on room air shows an oxygen saturation of 82%. Auscultation of the chest shows coarse crackles in both lungs and a diastolic murmur at the cardiac apex. Despite appropriate lifesaving measures, he dies. A photomicrograph of a section of myocardium obtained at autopsy is shown. Which of the following is the most likely underlying cause of this patient's cardiac disease?
A 61-year-old-male underwent deceased donor liver transplantation 3 weeks ago. During his follow up visit he complains of nausea and abdominal pain. He has been taking all of his medications as prescribed. He has a history of alcohol abuse and his last drink was one year ago. He does not smoke cigarettes and lives at home with his wife. On physical examination temperature is 98.6°F (37°C), blood pressure is 115/80 mmHg, pulse is 90/min, respirations are 18/min, and pulse oximetry is 99% on room air. He has scleral icterus and a positive fluid wave. Liver function tests are as follows: Alkaline phosphatase: 110 U/L Aspartate aminotransferase (AST, GOT): 100 U/L Alanine aminotransferase (ALT, GPT): 120 U/L Bilirubin total: 2.2 mg/dL Liver biopsy shows mixed dense interstitial lymphocytic infiltrates in the portal triad. What is the mechanism of this reaction?
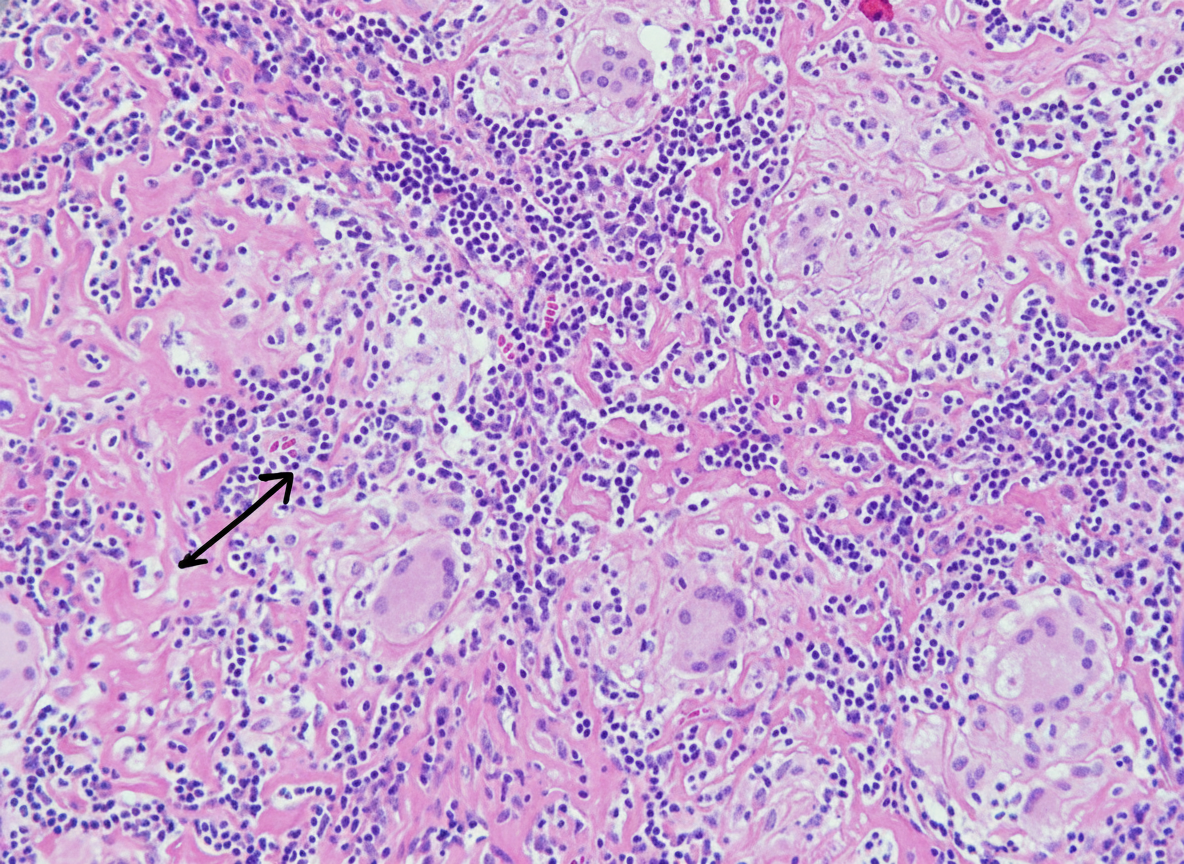
A 32-year-old man who recently emigrated from Somalia comes to the physician because of a 4-week history of fever, cough, and chest pain. He has had a 5-kg (11-lb) weight loss over the last 3 months despite no changes in appetite. His temperature is 38.1°C (100.6°F). Physical examination shows enlarged cervical lymph nodes. The lungs are clear to auscultation. The results of an interferon-γ release assay are positive. An x-ray of the chest shows bilateral mediastinal lymphadenopathy. A transbronchial needle aspiration biopsy of a mediastinal lymph node is performed; a photomicrograph of the specimen is shown. The structure indicated by the arrow is most likely comprised of which of the following types of cells?
A 23-year-old woman comes to the physician because of a 5-month history of a pruritic rash on the bilateral upper extremities. She has no history of serious illness and takes no medications. A skin biopsy of the rash shows intraepidermal accumulation of edematous fluid and widening of intercellular spaces between keratinocytes. Which of the following is the most likely diagnosis?
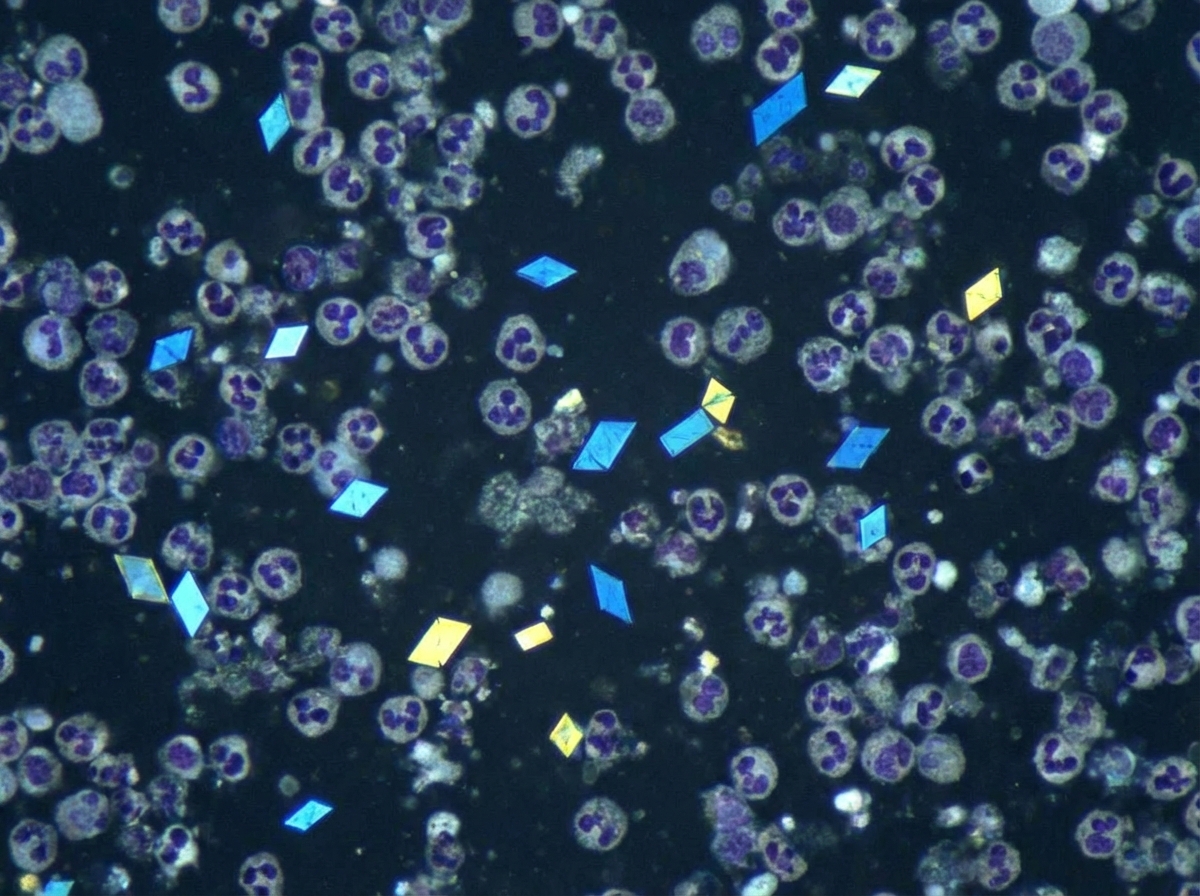
A 62-year-old man comes to the physician because of a swollen and painful right knee for the last 3 days. He has no history of joint disease. His vital signs are within normal limits. Examination shows erythema and swelling of the right knee, with limited range of motion due to pain. Arthrocentesis of the right knee joint yields 7 mL of cloudy fluid with a leukocyte count of 29,000/mm3 (97% segmented neutrophils). Compensated polarized light microscopy of the aspirate is shown. Which of the following is the most likely underlying mechanism of this patient's knee pain?
A 27-year-old woman presents to the emergency department for fever and generalized malaise. Her symptoms began approximately 3 days ago, when she noticed pain with urination and mild blood in her urine. Earlier this morning she experienced chills, flank pain, and mild nausea. Approximately 1 month ago she had the "flu" that was rhinovirus positive and was treated with supportive management. She has a past medical history of asthma. She is currently sexually active and uses contraception inconsistently. She occasionally drinks alcohol and denies illicit drug use. Family history is significant for her mother having systemic lupus erythematosus. Her temperature is 101°F (38.3°C), blood pressure is 125/87 mmHg, pulse is 101/min, and respirations are 18/min. On physical examination, she appears uncomfortable. There is left-sided flank, suprapubic, and costovertebral angle tenderness. Urine studies are obtained and a urinalysis is demonstrated below: Color: Amber pH: 6.8 Leukocyte: Positive Protein: Trace Glucose: Negative Ketones: Negative Blood: Positive Nitrite: Positive Leukocyte esterase: Positive Specific gravity: 1.015 If a renal biopsy is performed in this patient, which of the following would most likely be found on pathology?
A previously healthy 46-year-old woman comes to her physician because of an itchy rash on her legs. She denies any recent trauma, insect bites, or travel. Her vital signs are within normal limits. Examination of the oral cavity shows white lace-like lines on the buccal mucosa. A photograph of the rash is shown. A biopsy specimen of the skin lesion is most likely to show which of the following?

A 45-year-old immigrant presents with unintentional weight loss, sleep hyperhidrosis, and a persistent cough. He says these symptoms have been present for quite some time. Upon imaging, many granulomas in the upper lobes are present. It is noted that these apical granulomas have centers of necrosis that appear cheese-like in appearance. Encircling the area of necrosis are large cells with cytoplasms pale in color. Of the following surface markers, which one is most closely associated with these cells?
Practice by Chapter
Acute inflammation mechanisms
Practice Questions
Vascular changes in inflammation
Practice Questions
Chemical mediators of inflammation
Practice Questions
Cellular components of inflammation
Practice Questions
Resolution of acute inflammation
Practice Questions
Chronic inflammation
Practice Questions
Granulomatous inflammation
Practice Questions
Systemic effects of inflammation
Practice Questions
Patterns of inflammatory response
Practice Questions
Inflammatory markers in laboratory testing
Practice Questions
Anti-inflammatory therapies
Practice Questions
Wound healing and repair
Practice Questions
Abnormalities in wound healing
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app