
Inflammation — MCQs

On this page
A 10-year-old boy presents with sudden shortness of breath. The patient’s mother says he was playing in the school garden 2 hours ago and suddenly started to complain of abdominal pain and vomited a few times. An hour later, he slowly developed a rash that involved his chest, arms, and legs, and his breathing became faster, with audible wheezing. He has no significant past medical history. His temperature is 37.0°C (98.6°F), blood pressure is 100/60 mm Hg, pulse is 130/min, and respirations are 25/min. On physical examination, there is a rash on his right arm (shown in the image, below). Which of the following cells will mainly be found in this patient if a histological sample is taken from the site of the skin lesion 4 hours from now?

A 27-year-old man comes to the physician because of multiple, dry, scaly lesions on his elbows. The lesions appeared 4 months ago and have progressively increased in size. They are itchy and bleed when he scratches them. There is no associated pain or discharge. He was diagnosed with HIV infection 6 years ago. He has smoked a pack of cigarettes daily for the past 10 years. Current medications include raltegravir, lamivudine, abacavir, and cotrimoxazole. An image of the lesions is shown. His CD4+ T-lymphocyte count is 470/mm3 (normal ≥ 500). Which of the following is the most likely cause of this patient's skin findings?

A 37-year-old woman presents to the occupational health clinic for a new employee health screening. She has limited medical records prior to her immigration to the United States several years ago. She denies any current illness or significant medical history. Purified protein derivative (PPD) is injected on the inside of her left forearm for tuberculosis (TB) screening. Approximately 36 hours later, the patient comes back to the occupational health clinic and has an indurated lesion with bordering erythema measuring 15 mm in diameter at the site of PPD injection. Of the following options, which is the mechanism of her reaction?
A 22-year-old woman comes to the physician because of pain and swelling of her left foot. Three days ago, she cut her foot on an exposed rock at the beach. Her temperature is 37.7°C (100°F). Examination of the left foot shows edema around a fluctuant erythematous lesion on the lateral foot. Which of the following is most likely the primary mechanism for the development of edema in this patient?
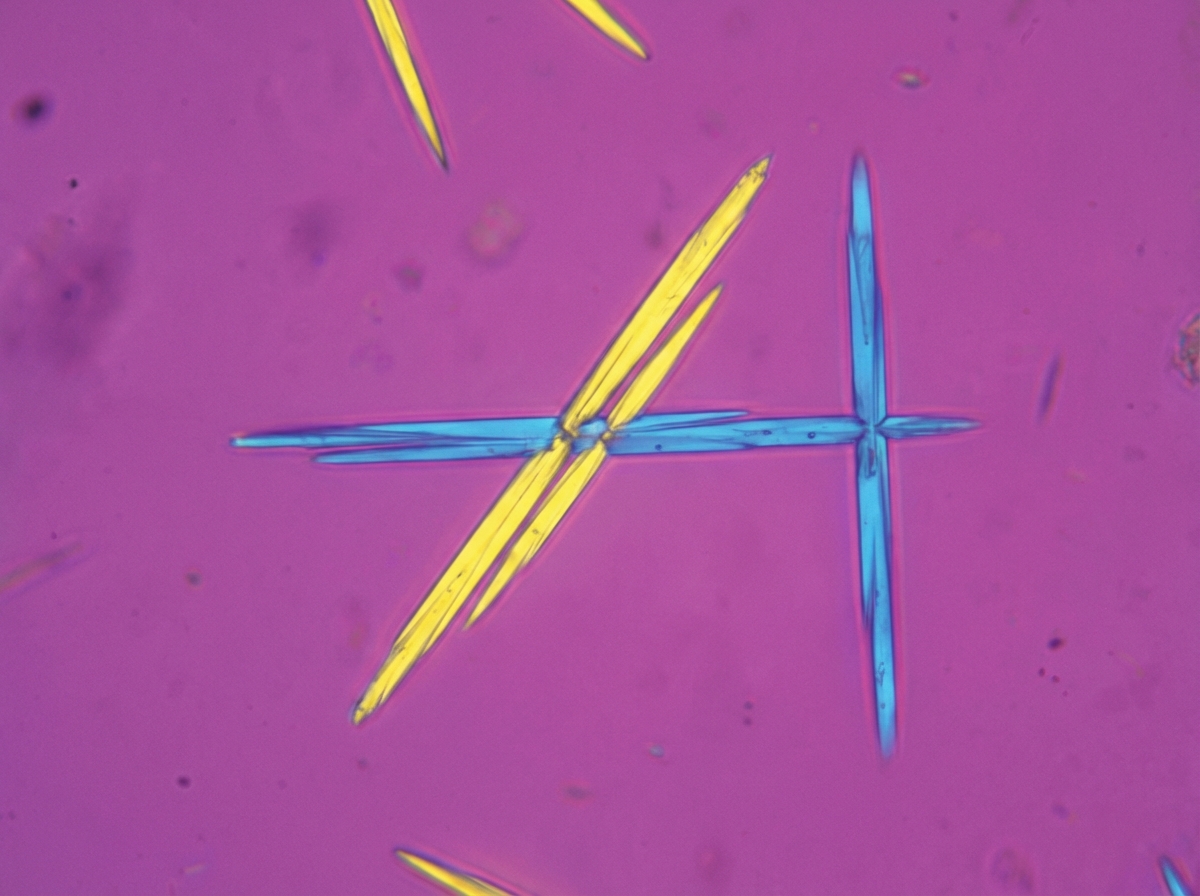
A 45-year-old construction worker presents to his primary care physician with a painful and swollen wrist joint. A joint aspiration shows crystals, which are shown in the accompanying picture. Which of the following is the most likely diagnosis?
A 23-year-old woman comes to the physician because of right-sided blurry vision and eye pain for 4 days. She has a 6-day history of low-grade fever, headache, and malaise. One year ago, she was diagnosed with Crohn disease. Her only medication is prednisone. Her temperature is 38°C (100.4°F), pulse is 84/min, and blood pressure is 112/75 mm Hg. The right eyelid is erythematous and tender; there are multiple vesicles over the right forehead and the tip of the nose. Visual acuity is 20/20 in the left eye and 20/80 in the right eye. Extraocular movements are normal. The right eye shows conjunctival injection and reduced corneal sensitivity. Fluorescein staining shows a corneal lesion with a tree-like pattern. Which of the following is the most likely diagnosis?
A 4-year-old Caucasian boy is brought by his mother to the pediatrician with a red and swollen elbow. He was playing outside a few days prior to presentation when he fell and lightly scraped his elbow on the sidewalk. He was born at 34 weeks' gestation and was in the neonatal ICU for 2 days. His temperature is 102.1°F (38.9°C), blood pressure is 105/65 mmHg, pulse is 110/min, and respirations are 20/min. On exam, he has a swollen, erythematous, fluctuant, and exquisitely tender mass on his right elbow. There is expressible purulence coming from his wound. A peripheral blood smear in this patient would most likely reveal which of the following findings?
Two days after being admitted for acute myocardial infarction, a 61-year-old man has sharp, substernal chest pain that worsens with inspiration and improves when leaning forward. Cardiac examination shows a scratchy sound best heard over the left sternal border. Histopathological examination of the infarcted myocardial tissue is most likely to show which of the following findings?
A 42-year-old man comes to the physician because of a 6-week history of intermittent fever, abdominal pain, bloody diarrhea, and sensation of incomplete rectal emptying. He also has had a 4.5-kg (10-lb) weight loss over the past 3 months. Abdominal examination shows diffuse tenderness. Colonoscopy shows circumferential erythematous lesions that extend without interruption from the anal verge to the cecum. A biopsy specimen taken from the rectum shows mucosal and submucosal inflammation with crypt abscesses. This patient is most likely at risk of developing colon cancer with which of the following characteristics?
A 42-year-old woman comes to the clinic with a complaint of a severely itchy and painful rash on her hands and legs for a day. On further questioning, she revealed that she loves nature and goes on trekking to the woods frequently. She just returned from a similar trip, 2 days ago. On physical examination, a prominent rash along with multiple blisters is noted on the ventral aspect of her right forearm. A photograph of the rash is shown. Which of the following is the most likely reaction that the patient is experiencing?

Practice by Chapter
Acute inflammation mechanisms
Practice Questions
Vascular changes in inflammation
Practice Questions
Chemical mediators of inflammation
Practice Questions
Cellular components of inflammation
Practice Questions
Resolution of acute inflammation
Practice Questions
Chronic inflammation
Practice Questions
Granulomatous inflammation
Practice Questions
Systemic effects of inflammation
Practice Questions
Patterns of inflammatory response
Practice Questions
Inflammatory markers in laboratory testing
Practice Questions
Anti-inflammatory therapies
Practice Questions
Wound healing and repair
Practice Questions
Abnormalities in wound healing
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app