
Inflammation — MCQs

On this page
A 68-year-old woman with osteoarthritis comes to the physician because of a swollen and painful right knee for the past 2 days. Temperature is 37°C (98.6°F). Examination shows erythema and swelling of the right knee with a normal range of motion. An x-ray of the right knee shows punctate radiodensities in both menisci and in the joint capsule. Arthrocentesis of the right knee joint yields 5 mL of cloudy fluid with a leukocyte count of 27,000/mm3. Which of the following is the most likely underlying mechanism of this patient's knee pain?
A 36-year-old woman presents with thyroid swelling. She has been healthy until now and follows all the healthcare precautions except for missing a flu shot this year. On physical examination, the thyroid gland is diffusely enlarged and tender to palpation. Laboratory findings show a decreased serum TSH level and elevated erythrocyte sedimentation rate. Which of the following histopathologic findings would most likely be found in the thyroid gland of this patient?
A 32-year-old woman presents to her primary care provider complaining of a psoriatic flare that has worsened over the past 2 days. The patient states that her psoriasis is normally well-controlled. She also complains of some fatigue and states that she has recently developed pain and tenderness in the joints of her hands with the right hand being more tender than the left. Her hands are stiff in the morning, and sometimes her fingers swell up. She attributes these changes to her new job where she constantly uses her hands to manufacture cabinets. Physical exam reveals plaques with silvery scale on her elbows and knees. The distal joints of her right hand are mildly swollen and the nails on both hands appear pitted. What is the most likely pathogenesis of her joint pain?
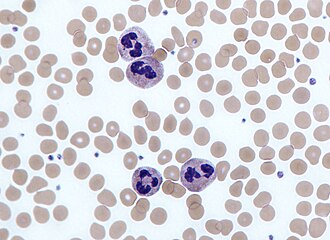
A 14-year-old girl presents with pain in the right lower quadrant of her abdomen. She describes the pain as sudden, severe, colicky, and associated with nausea and vomiting. Physical exam reveals tachycardia and severe tenderness to palpation with rebound in the right iliac region. Emergency laparotomy is performed which reveals an inflamed appendix. A presurgical blood cell count shows an increase in the number of cells having a multilobed nucleus and multiple cytoplasmic granules as shown in the image below. Which of the following is the main function of these cells?
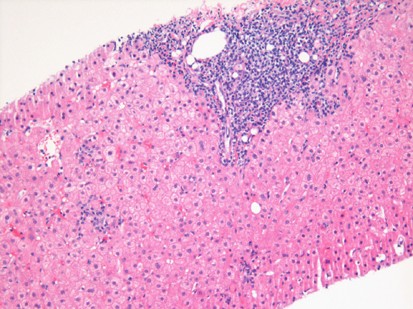
A 57-year-old man comes to the physician for a follow-up visit. Serum studies show: AST 134 U/L ALT 152 U/L Hepatitis B surface antigen Positive A photomicrograph of the microscopic findings of a liver biopsy is shown. These biopsy findings are most characteristic of which of the following types of inflammatory reactions?
A 37-year-old man presents to his primary care physician because he has had constipation for the last several weeks. He has also been feeling lethargic and complains that this winter has been particularly cold. He also complains that he has been gaining weight despite no change in his normal activities. He reveals that two months prior to presentation he had what felt like the flu for which he took Tylenol and did not seek medical attention. Several days after this he developed anterior neck pain. Which of the following findings would most likely be seen on biopsy of this patient's abnormality?
A 23-year-old woman comes to the physician for evaluation of two masses on her right auricle for several months. The masses appeared a few weeks after she had her ear pierced and have increased in size since then. A photograph of her right ear is shown. Which of the following is the most likely cause of these findings?

A 4-year-old male is accompanied by his mother to the pediatrician. His mother reports that over the past two weeks, the child has had intermittent low grade fevers and has been more lethargic than usual. The child’s past medical history is notable for myelomeningocele complicated by lower extremity weakness as well as bowel and bladder dysfunction. He has been hospitalized multiple times at an outside facility for recurrent urinary tract infections. The child is in the 15th percentile for both height and weight. His temperature is 100.7°F (38.2°C), blood pressure is 115/70 mmHg, pulse is 115/min, and respirations are 20/min. Physical examination is notable for costovertebral angle tenderness that is worse on the right. Which of the following would most likely be found on biopsy of this patient’s kidney?
A 68-year-old man is admitted to the emergency department after 2 days of difficulty breathing and fever. His past medical history is significant for hypertension and benign prostate hypertrophy. He takes hydrochlorothiazide and tamsulosin. He also admits to drinking alcohol on the weekends and a half pack a day smoking habit. Upon admission, he is found to have blood pressure of 125/83 mm Hg, pulse of 88/min, a respiratory rate of 28/min, and a temperature of 38.9°C (102°F). On physical exam breath sounds are decreased at the left pulmonary base. A chest x-ray reveals consolidation in the left lower lobe. Additional laboratory tests demonstrate leukocytosis, elevated C-reactive protein, a serum creatinine (Cr) of 8.0 mg/dL, and a blood urea nitrogen (BUN) of 32 mg/dL. The patient is admitted to the hospital and started on cefepime and clarithromycin. His dyspnea slowly improves after 48 hours, however, his body temperature remains at 39°C (102.2°F). Recent laboratory tests show reduced C-reactive protein levels, a Cr of 1.8 mg/dL and a BUN of 35 mg/dL. A urinalysis is ordered. Which of the following would you expect to find in this patient’s urine?
A 69-year-old diabetic woman comes to the emergency department due to right flank pain for 10 days. Her right flank pain is radiating towards her groin and is associated with fever and chills. The pain is exacerbated with hip extension. She feels fatigued and is lying on her left side with her right hip flexed. The CT guided percutaneous drainage reveals 900 ml of greenish pus. The vital signs include blood pressure 145/75 mm Hg, pulse rate 96/min, temperature 36.9°C (98.4°F), respiratory rate 16/min, and the oxygen saturation is 95%. The complete blood count shows the following results upon admission: CBC results Leukocytes 16,600/mm3 Neutrophils 80% Lymphocytes 16% Eosinophils 1% Basophils 1% Monocyte 2% Hemoglobin 7.6 g/dL Creatinine 0.8 mg/dL BUN 15 mg/dL Which of the following processes most likely could have occurred?
Practice by Chapter
Acute inflammation mechanisms
Practice Questions
Vascular changes in inflammation
Practice Questions
Chemical mediators of inflammation
Practice Questions
Cellular components of inflammation
Practice Questions
Resolution of acute inflammation
Practice Questions
Chronic inflammation
Practice Questions
Granulomatous inflammation
Practice Questions
Systemic effects of inflammation
Practice Questions
Patterns of inflammatory response
Practice Questions
Inflammatory markers in laboratory testing
Practice Questions
Anti-inflammatory therapies
Practice Questions
Wound healing and repair
Practice Questions
Abnormalities in wound healing
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app