
Secondary immunodeficiencies — MCQs

A 13-month-old boy is referred to an immunologist with recurrent otitis media, bacterial sinus infections, and pneumonia, which began several months earlier. He is healthy now, but the recurrent nature of these infections are troubling to his parents and they are hoping to find a definitive cause. The boy was born at 39 weeks gestation via spontaneous vaginal delivery. He is up to date on all vaccines and is meeting all developmental milestones. The patient has five older siblings, but none of them had similar recurrent illnesses. Clinical pathology results suggest very low levels of serum immunoglobulin. As you discuss options for diagnosis with the patient’s family, which of the following tests should be performed next?
A 3-month-old boy presents to his pediatrician with persistent diarrhea, oral candidiasis, and signs and symptoms of respiratory syncytial virus (RSV) pneumonia. He is very lean with weight in the 10th percentile. His blood pressure is 105/64 mm Hg and heart rate is 84/min. He is being evaluated for an immunodeficiency. Laboratory results for HIV are negative by polymerase chain reaction (PCR). Which of the following is the most likely cause of this child’s presentation?
A young infant is brought to an immunologist because of recurrent infections, which have not resolved despite appropriate medical treatment. On reviewing her medical history, the immunologist notes that the child has had frequent disseminated mycobacterial infections. He suspects a possible immunodeficiency. What is the most likely cause of this patient's immunodeficiency?
A 37-year old man is being evaluated due to a recent history of fatigue that started 3 weeks ago. The patient presents with a history of HIV, which was first diagnosed 7 years ago. He has been on an antiretroviral regimen and takes it regularly. His CD4+ count is 350 cells/mm3. According to the patient, his partner passed away from a "blood cancer", and he is worried that his fatigue might be connected to a similar pathology. The physician clarifies that there is an increased risk for HIV patients to develop certain kinds of lymphomas. Which one of the conditions below is the patient more likely to develop based on his medical history?
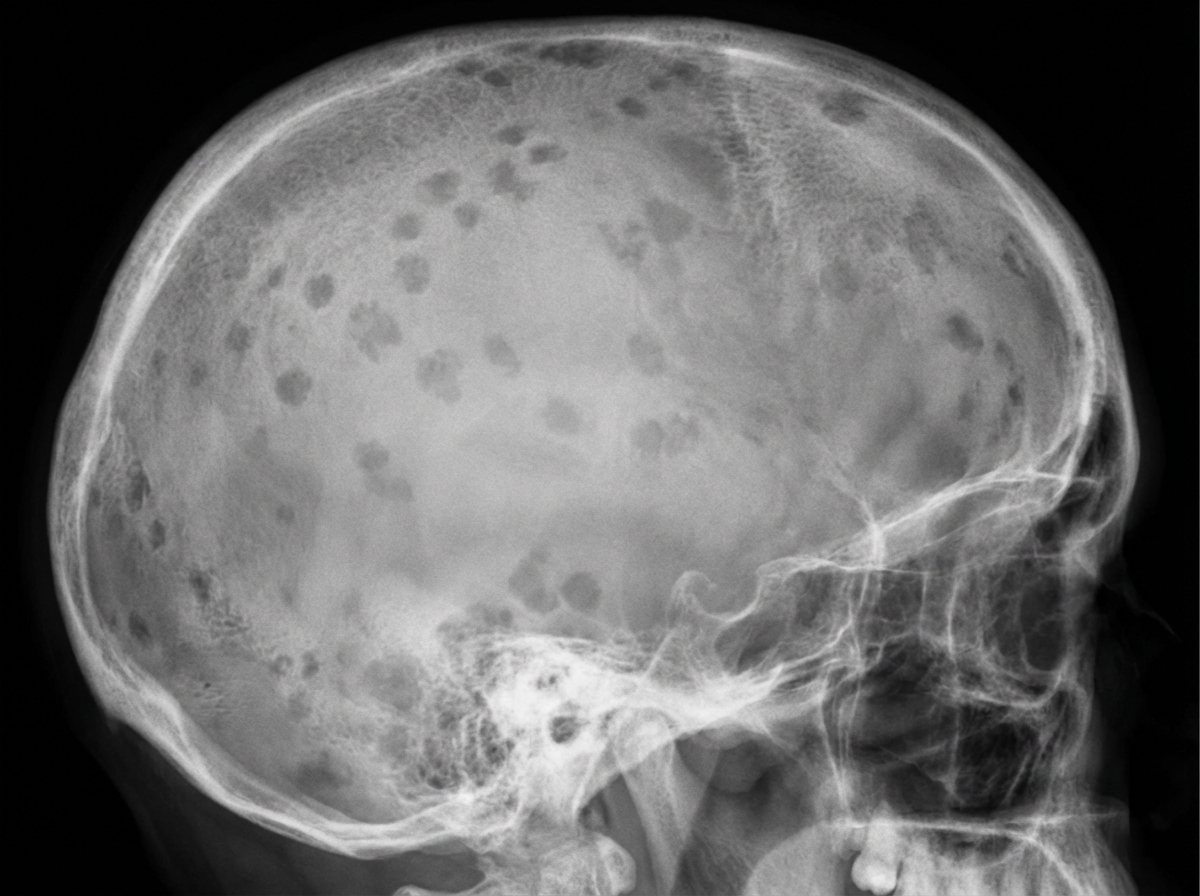
A 71-year-old African American man is brought to the emergency department with a worsening productive cough and dyspnea for 2 days. He has had generalized bone pain for 2 months. He was admitted for pyelonephritis last month. He also received outpatient treatment for pneumonia almost 2 months ago. Over the past 2 months, he has been taking over-the-counter ibuprofen for pain as needed. He appears anxious. The vital signs include: temperature 38.8°C (101.8°F), pulse 95/min, respiratory rate 20/min, and blood pressure 155/90 mm Hg. The conjunctivae are pale. Crackles are heard in the right lower lobe. The cardiac examination shows no abnormalities. The laboratory studies show the following: Hemoglobin 9 g/dL Mean corpuscular volume 95 μm3 Leukocyte count 13,500/mm3 Segmented neutrophils 75% Lymphocytes 25% Platelet count 240,000/mm3 ESR 85 mm/hr Serum Na+ 135 mEq/L K+ 4.2 mEq/L Cl− 113 mEq/L HCO3− 20 mEq/L Ca+ 12.4 mg/dL Albumin 4 g/dL Urea nitrogen 38 mg/dL Creatinine 2.2 mg/dL A chest X-ray shows a right lower lobe opacity and blurring of the ipsilateral diaphragmatic dome. Skull and pelvic X-rays are performed (see image). Which of the following is the most likely underlying cause of this patient’s recent infections?
A 33-year-old man is brought into the emergency department with fever, lethargy, and confusion. He is a cachectic man in acute distress, unable to respond to questions or follow commands. His friend confides that the patient has been sexually active with multiple male partners and was diagnosed with HIV several months ago, but was lost to follow up. Based on prior records, his most recent CD4 count was 65 cells/uL. Which of the following is the most appropriate next step in management?
You are seeing a 4-year-old boy in clinic who is presenting with concern for a primary immune deficiency. He has an unremarkable birth history, but since the age of 6 months he has had recurrent otitis media, bacterial pneumonia, as well as two episodes of sinusitis, and four episodes of conjunctivitis. He has a maternal uncle who died from sepsis secondary to H. influenza pneumonia. If you drew blood work for diagnostic testing, which of the following would you expect to find?
An investigator is studying the mechanism of HIV infection in cells obtained from a human donor. The effect of a drug that impairs viral fusion and entry is being evaluated. This drug acts on a protein that is cleaved off of a larger glycosylated protein in the endoplasmic reticulum of the host cell. The protein that is affected by the drug is most likely encoded by which of the following genes?
A 1-year-old infant is brought to the emergency department by his parents because of fever and rapid breathing for the past 2 days. He had a mild seizure on the way to the emergency department and developed altered sensorium. His mother states that the patient has had recurrent respiratory infections since birth. He was delivered vaginally at term and without complications. He is up to date on his vaccines and has met all developmental milestones. His temperature is 37.0°C (98.6°F), pulse rate is 200/min, and respirations are 50/min. He is lethargic, irritable, and crying excessively. Physical examination is notable for a small head, an elongated face, broad nose, low set ears, and cleft palate. Cardiopulmonary exam is remarkable for a parasternal thrill, grade IV pansystolic murmur, and crackles over both lung bases. Laboratory studies show hypocalcemia and lymphopenia. Blood cultures are drawn and broad-spectrum antibiotics are started, and the child is admitted to the pediatric intensive care unit. The intensivist suspects a genetic abnormality and a fluorescence in situ hybridization (FISH) analysis is ordered which shows 22q11.2 deletion. Despite maximal therapy, the infant succumbs to his illness. The parents of the child request an autopsy. Which of the following findings is the most likely to be present on autopsy?
A 27-year-old woman presents to the emergency department complaining of a left-sided headache and right-sided blurry vision. She states that 2 weeks ago she developed dark urine and abdominal pain. She thought it was a urinary tract infection so she took trimethoprim-sulfamethoxazole that she had left over. She planned on going to her primary care physician today but then she developed headache and blurry vision so she came to the emergency department. The patient states she is otherwise healthy. Her family history is significant for a brother with sickle cell trait. On physical examination, there is mild abdominal tenderness, and the liver edge is felt 4 cm below the right costal margin. Labs are drawn as below: Hemoglobin: 7.0 g/dL Platelets: 149,000/mm^3 Reticulocyte count: 5.4% Lactate dehydrogenase: 3128 U/L Total bilirubin: 2.1 mg/dL Indirect bilirubin: 1.4 mg/dL Aspartate aminotransferase: 78 U/L Alanine aminotransferase: 64 U/L A peripheral smear shows polychromasia. A Doppler ultrasound of the liver shows decreased flow in the right hepatic vein. Magnetic resonance imaging of the brain is pending. Which of the following tests, if performed, would most likely identify the patient’s diagnosis?
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app