
Immune-related adverse events — MCQs

A 56-year-old African American presents to the emergency department due to abdominal pain, fatigue, and weight loss over the past 3 months. He has a long-standing history of chronic hepatitis B virus infection complicated by cirrhosis. On examination, he has jaundice, leg edema, and a palpable mass in the right upper abdominal quadrant. Abdominal ultrasound shows a 3-cm liver mass with poorly defined margins and coarse, irregular internal echoes. Blood investigations are shown: Aspartate aminotransferase (AST) 90 U/L Alanine aminotransferase (ALT) 50 U/L Total bilirubin 2 mg/dL Albumin 3 g/dL Alkaline phosphatase 100 U/L Alpha fetoprotein 600 micrograms/L Which of the following targeted agents is approved for advanced-stage hepatoma?
A 49-year-old man presents to a new primary care provider complaining of fatigue and occasional fever over the last month. These symptoms are starting to affect his job and he would like treatment. The physician runs a standard metabolic panel that shows elevated AST and ALT. The patient is then tested for hepatitis viruses. He is hepatitis C positive. The patient and his doctor discuss treatment options and agree upon pegylated interferon and oral ribavirin. Which side-effect is most likely while taking the ribavirin?
A 46-year-old male presents to his dermatologist for routine follow-up of his psoriasis. He was last seen in the office six months prior, at which time he started undergoing ultraviolet light therapy. He reports that he initially noticed an improvement in his symptoms but the effects were transient. He has also started noticing pain and stiffness in his fingers. His past medical history is notable for obesity and diabetes mellitus. He takes metformin. His temperature is 99°F (37.2°C), blood pressure is 130/80 mmHg, pulse is 80/min, and respirations are 16/min. Multiple plaques with scaling are noted on the extensor surfaces of the upper and lower extremities. The patient’s physician suggests stopping the ultraviolet light therapy and starting an injectable medication that acts as a decoy receptor for a pro-inflammatory cytokine. Which of the following is an adverse effect associated with the use of this medication?
A 38-year-old woman comes to the physician for a follow-up examination. Two years ago, she was diagnosed with multiple sclerosis. Three weeks ago, she was admitted and treated for right lower leg weakness with high-dose methylprednisone for 5 days. She has had 4 exacerbations over the past 6 months. Current medications include interferon beta and a multivitamin. Her temperature is 37°C (98.6°F), pulse is 90/min, and blood pressure is 116/74 mm Hg. Examination shows pallor of the right optic disk. Neurologic examination shows no focal findings. She is anxious about the number of exacerbations and repeated hospitalizations. She is counseled about the second-line treatment options available to her. She consents to treatment with natalizumab. However, she has read online about its adverse effects and is concerned. This patient is at increased risk for which of the following complications?
A 35-year-old man comes to the physician because of a 6-month history of fatigue and increased sweating at night. He says that he feels “constantly tired” and needs more rest than usual although he sleeps well. In the morning, his sheets are often wet and his skin is clammy. He has not had any sore throat, runny nose, or cough recently. He has not traveled anywhere. Over the past 4 months, he has had a 6.8-kg (15-lb) weight loss, despite having a normal appetite. He does not drink or urinate more than usual. He is 181 cm (5 ft 11 in) tall and weighs 72 kg (159 lb); BMI is 22 kg/m2. His temperature is 37.9°C (100.2°F), pulse is 65/min, and blood pressure is 120/70 mm Hg. Physical examination shows no abnormalities. An HIV screening test and confirmatory test are both positive. The CD4 count is 600 cells/μl and the viral load is 104 copies/mL. Treatment with lamivudine, zidovudine, and indinavir is begun. The patient is at greatest risk for which of the following adverse effects?
A 51-year-old woman with hyperlipidemia comes to the physician because of weakness for one month. At the end of the day, she feels too fatigued to cook dinner or carry a laundry basket up the stairs. She also complains of double vision after she reads for long periods of time. All of her symptoms improve with rest. Her only medication is pravastatin. Physical examination shows drooping of the upper eyelids. Strength is initially 5/5 in the upper and lower extremities but decreases to 4/5 after a few minutes of sustained resistance. Sensation to light touch is intact and deep tendon reflexes are normal. Which of the following best describes the pathogenesis of this patient's condition?
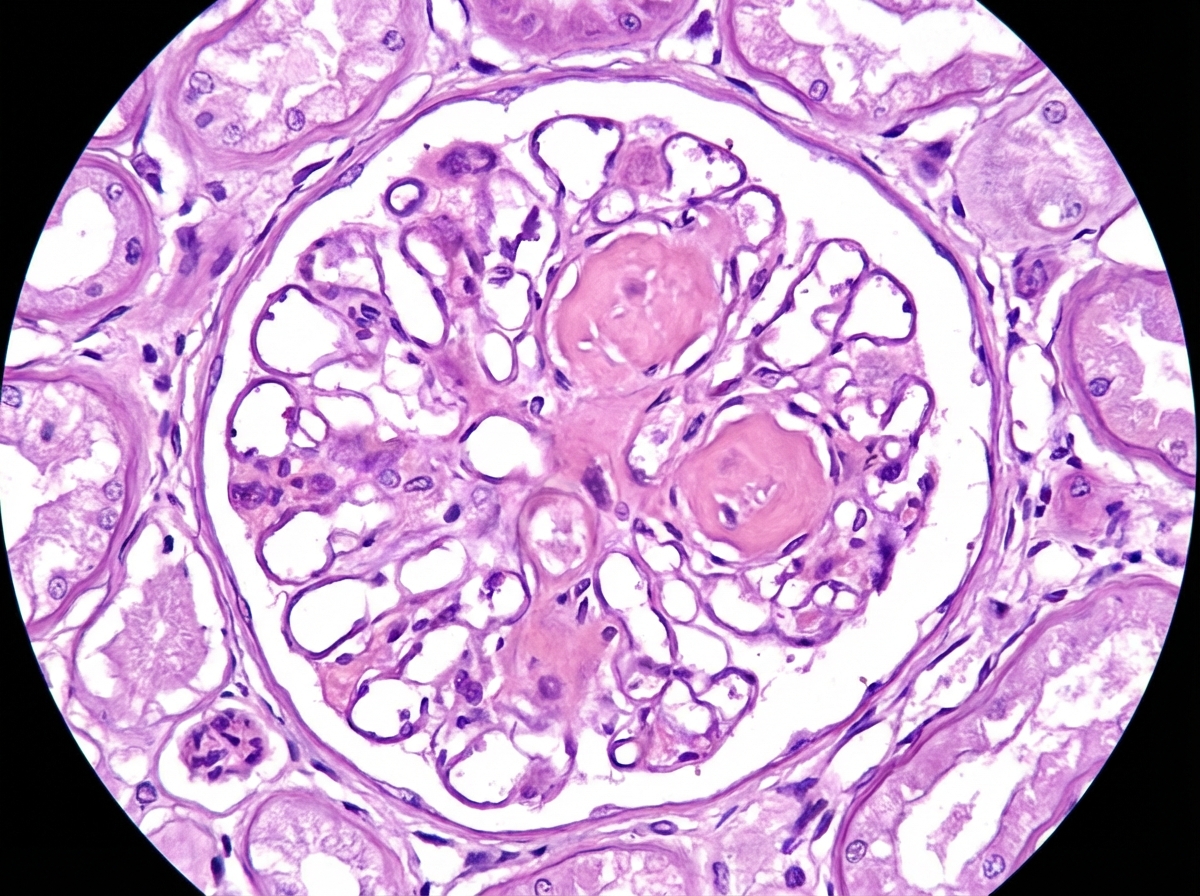
A 62-year-old man comes to the physician because of fatigue and decreased urine output for 2 weeks. He has not been to the physician for many years and takes no medications. Serum studies show a urea nitrogen concentration of 42 mg/dL and a creatinine concentration of 2.3 mg/dL. Urinalysis shows heavy proteinuria. A photomicrograph of a section of a kidney biopsy specimen is shown. Which of the following is the most likely underlying cause of this patient's symptoms?
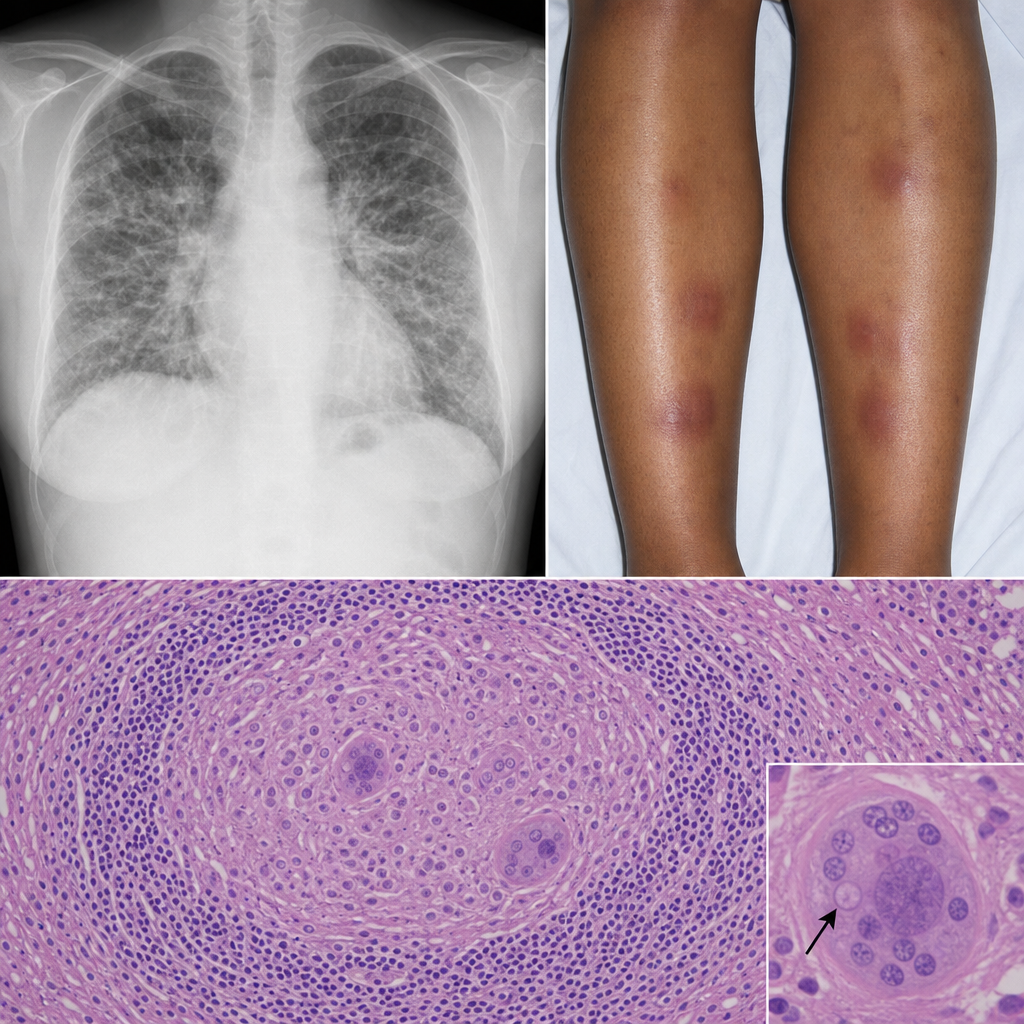
A 32-year-old Black woman with no occupational exposures presents with progressive dyspnea, fatigue, and bilateral ankle swelling. She also reports erythema nodosum on her shins. A chest radiograph shows bilateral hilar enlargement and diffuse interstitial infiltrates. Bronchoscopic biopsy is performed. The biopsy shows discrete, well-formed granulomas without central necrosis, surrounded by a rim of lymphocytes, with occasional Schaumann bodies and asteroid inclusions within giant cells. No organisms are identified on special stains. Which of the following best describes the predominant immunological mechanism driving this morphological pattern?
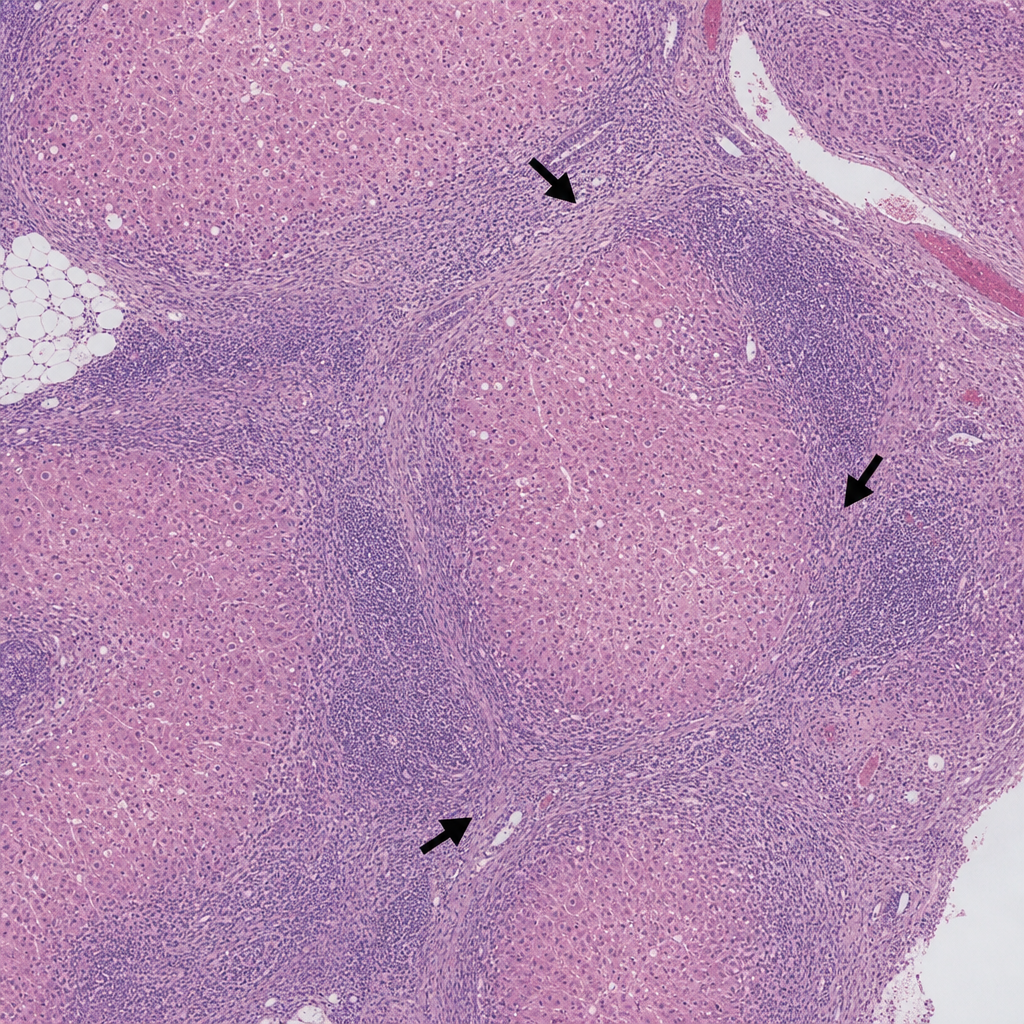
A 45-year-old woman presents with fatigue and jaundice. Serology is positive for anti-smooth muscle antibodies and elevated IgG. A liver biopsy is performed and shows a dense lymphoplasmacytic infiltrate expanding the portal tracts with interface hepatitis (piecemeal necrosis), plasma cell rosettes, and scattered acidophil bodies within the lobule. The lobular architecture is preserved. Which of the following findings, if present on the same biopsy, would most strongly support progression to an irreversible stage of this disease process?
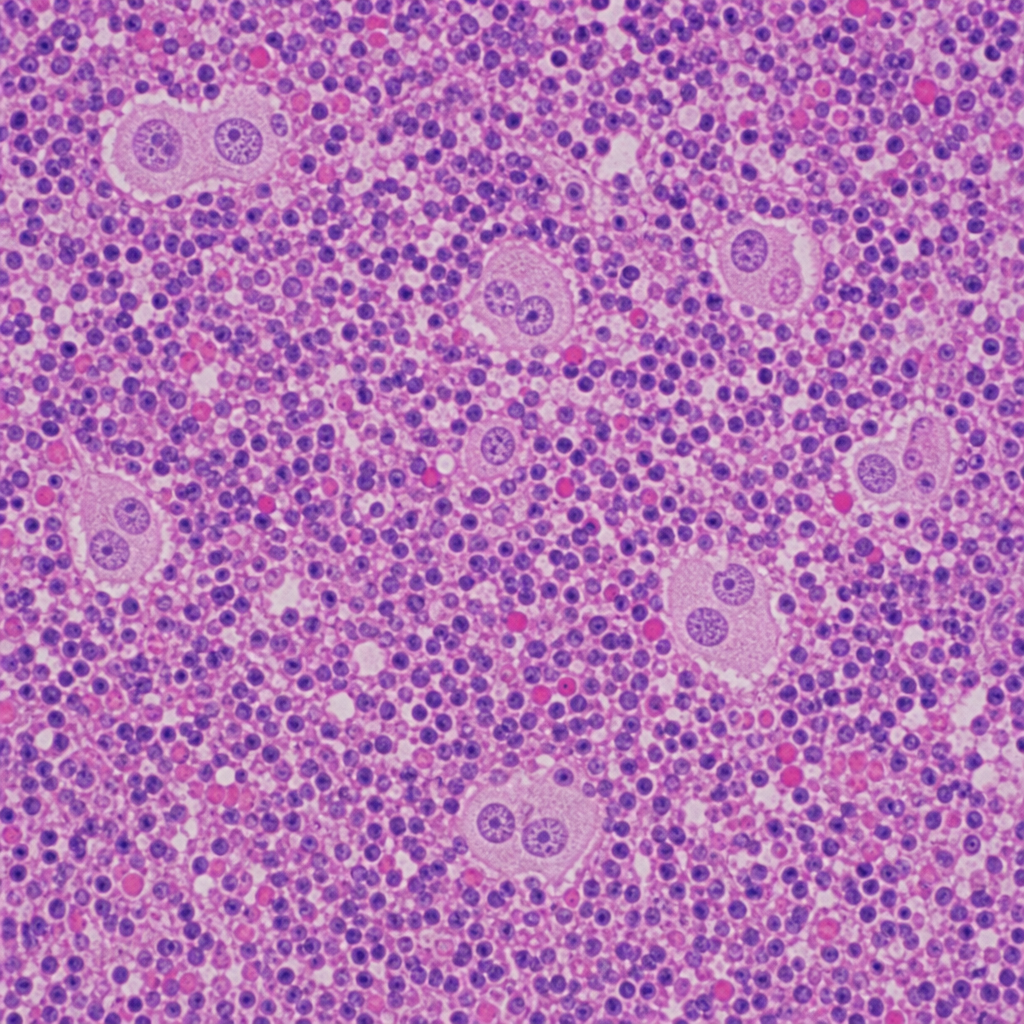
A 34-year-old woman presents with painless cervical lymphadenopathy, night sweats, and a 6 kg weight loss over 3 months. Excisional lymph node biopsy is performed. The photomicrograph demonstrates effacement of nodal architecture by a mixed inflammatory infiltrate of lymphocytes, plasma cells, eosinophils, and neutrophils. Scattered large binucleated cells with prominent eosinophilic 'owl-eye' nucleoli are identified; these cells are CD15+, CD30+, CD20−, and CD45−. A second population of mononuclear variants with similar nuclear features is also present. Which of the following most accurately characterizes the large binucleated cells in this biopsy?
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app