
Hematopathology — MCQs

On this page
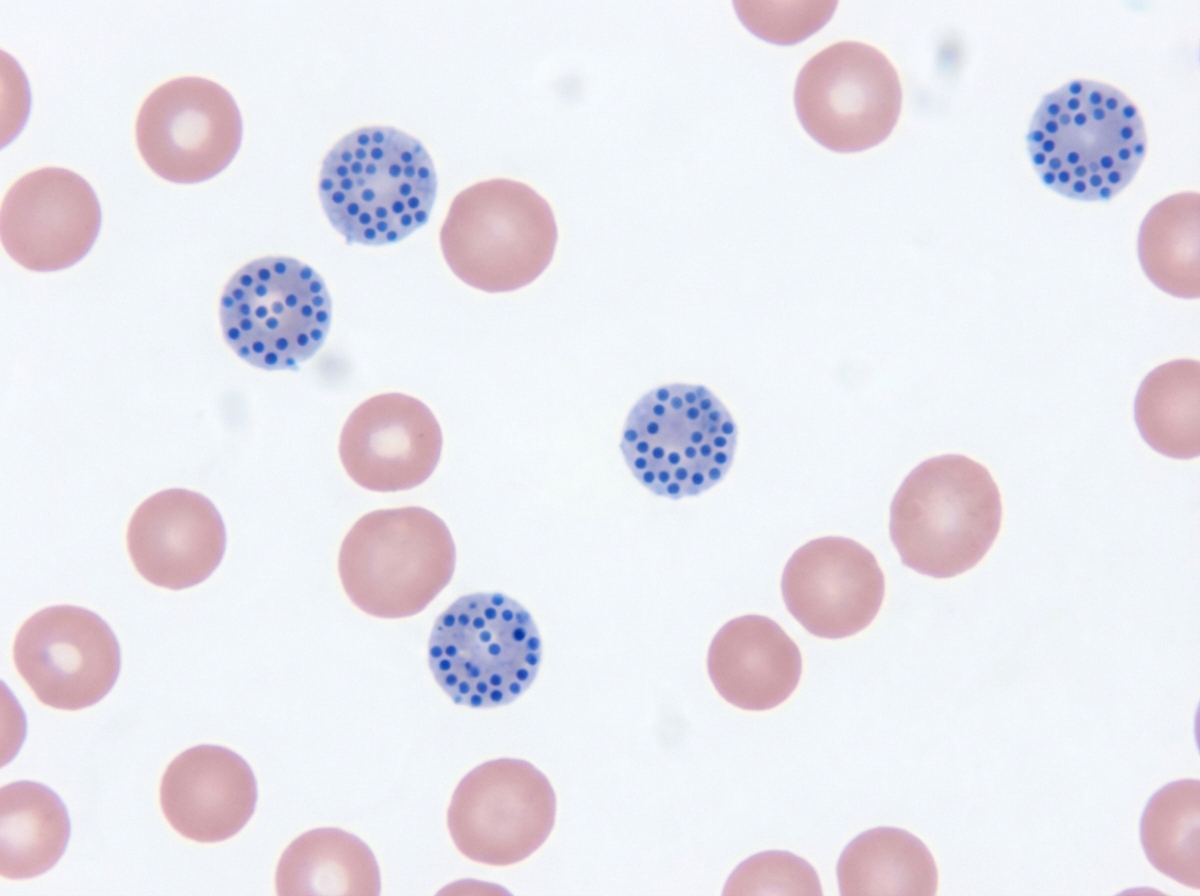
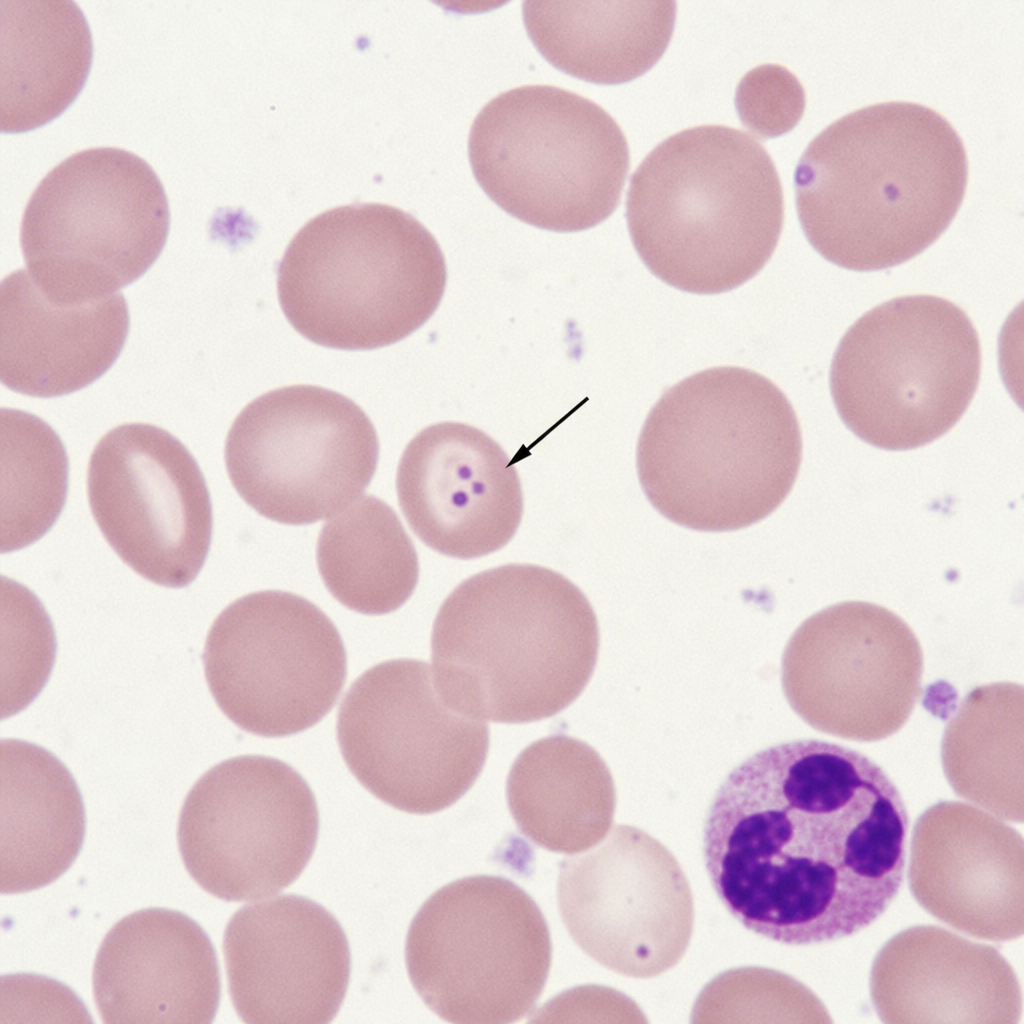
The following RBC inclusion is composed of:
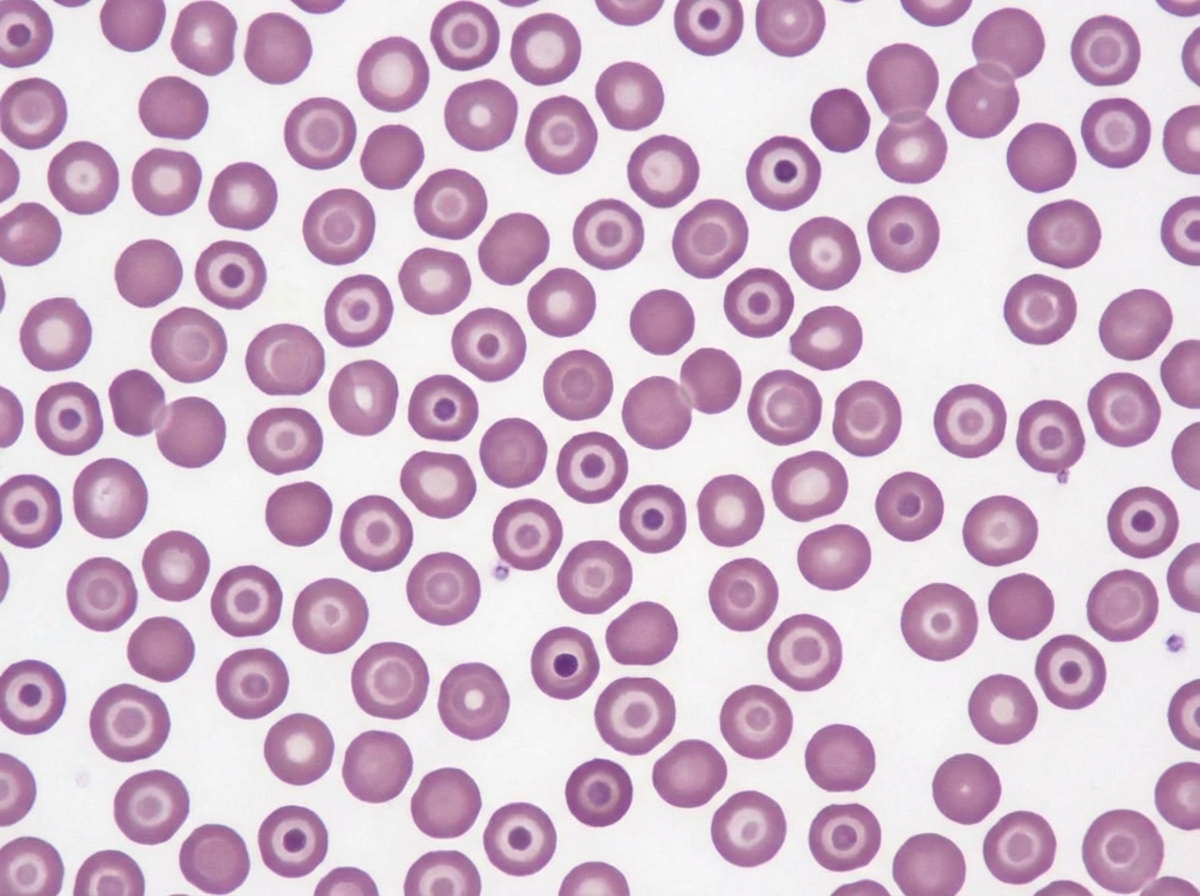
The following image shows presence of:
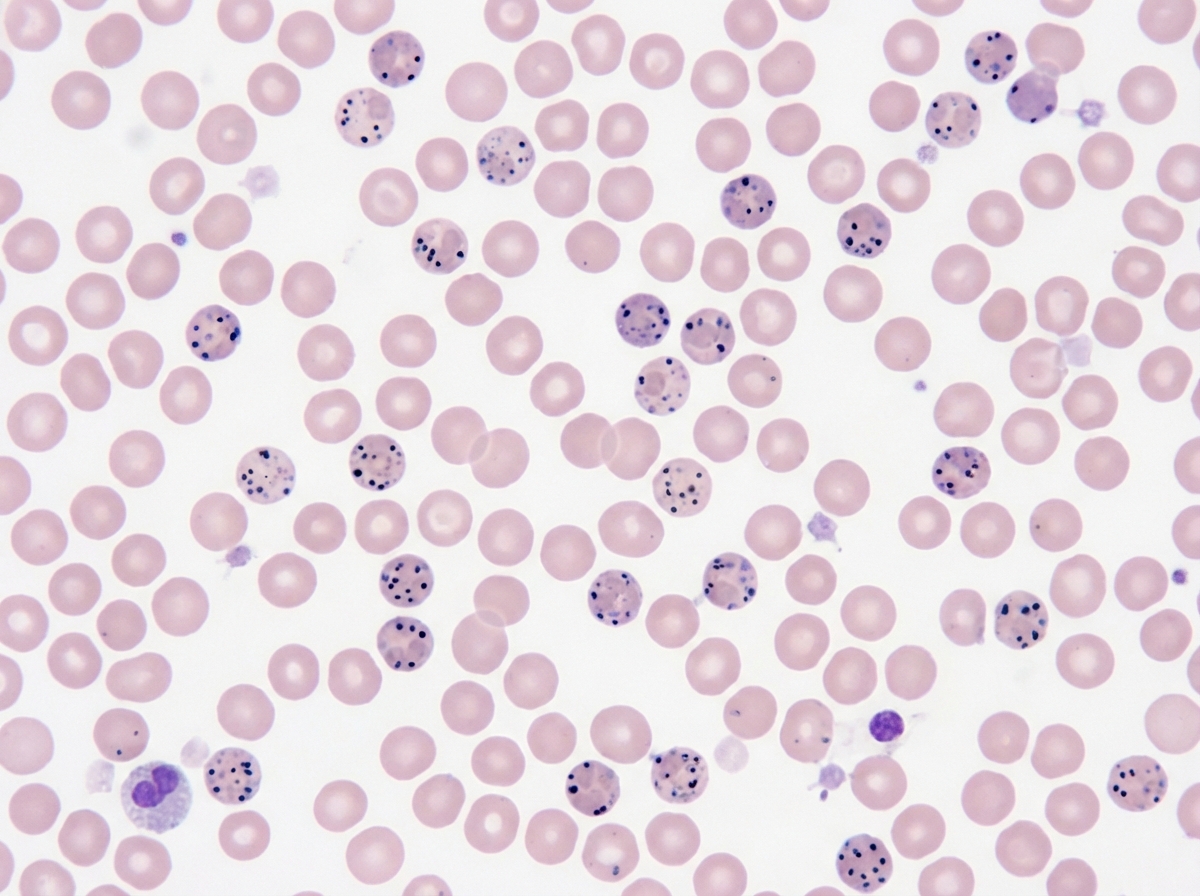
Which stain is preferred to diagnose these RBC inclusions seen in patients with HbH disease?
The diagnosis for the given presentation is:
A 6-year-old child presents with lethargy and abdominal pain. Hemoglobin is 8 g/dL with increased serum ferritin. Peripheral smear is shown. Which is correct about the image?
The following inclusions in multiple myeloma are called:
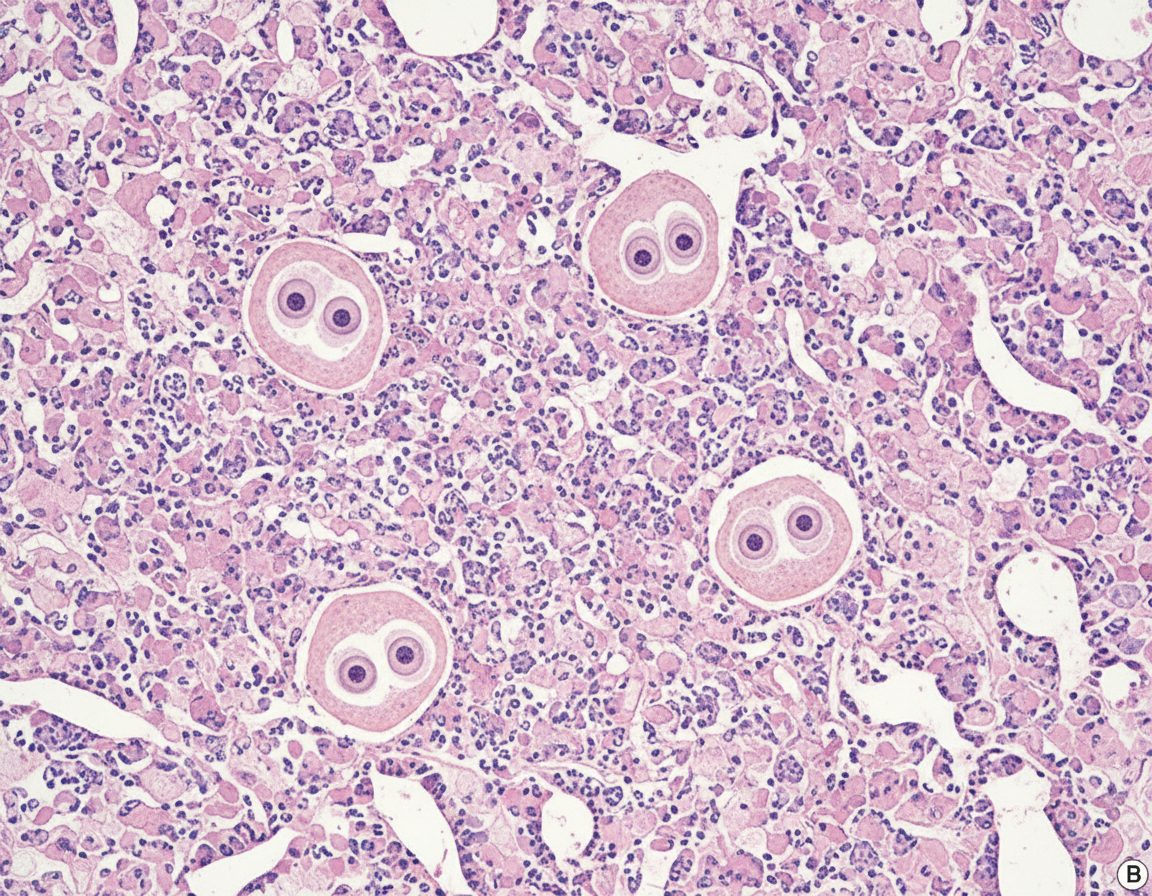
What is your diagnosis on the basis of image given below?
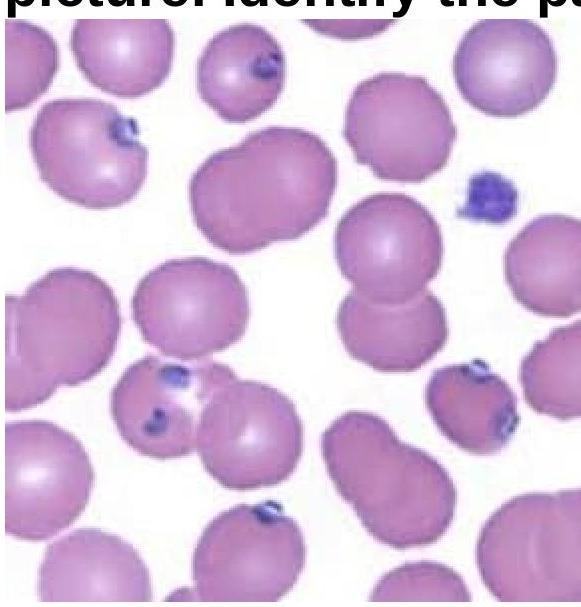
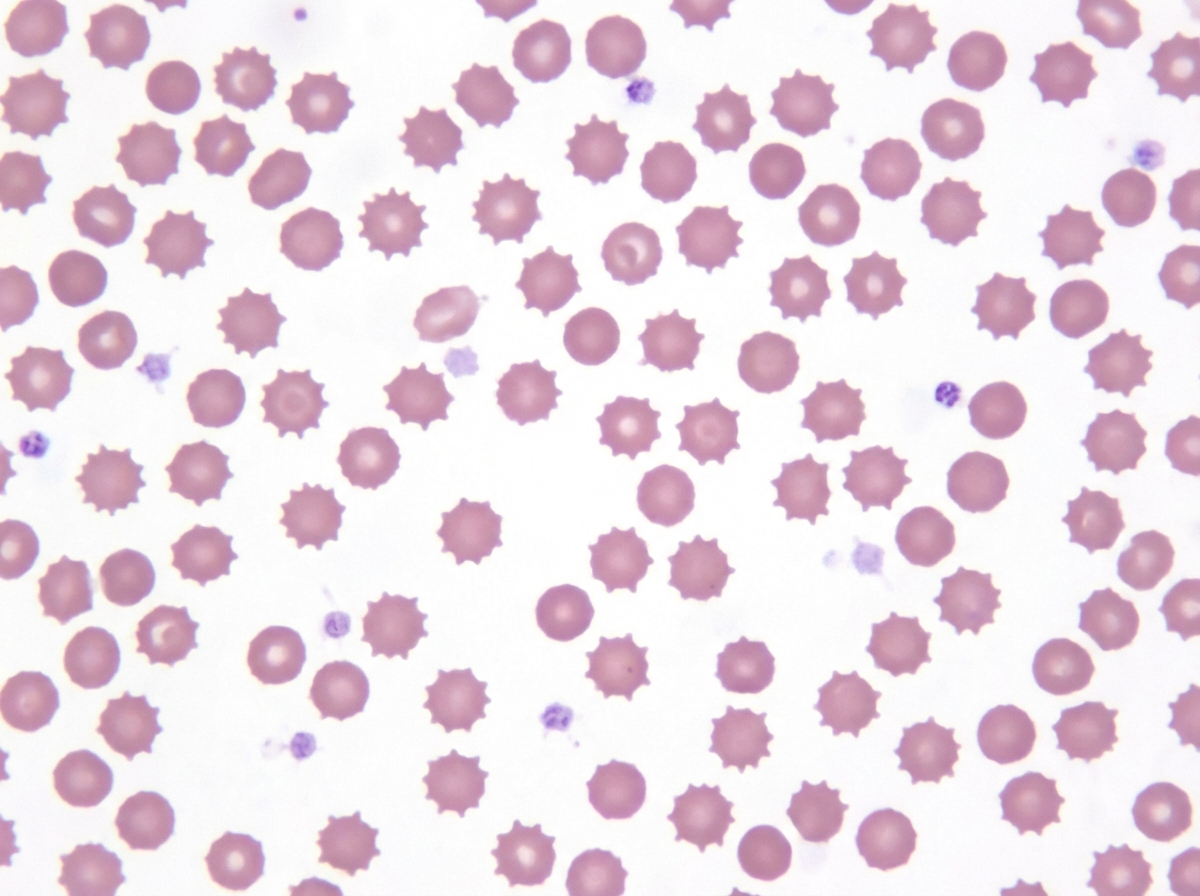
Identify the RBC shown in the figure:
All are true about the slide shown except:
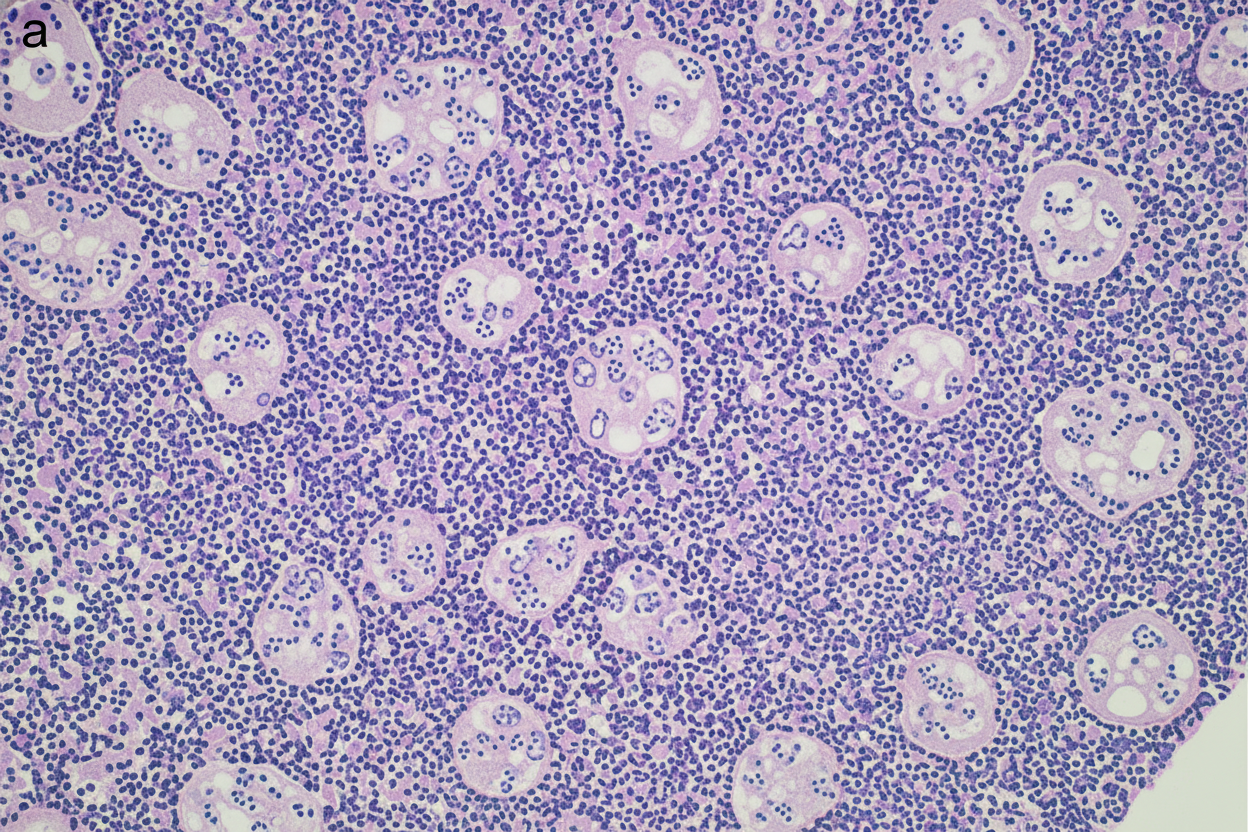
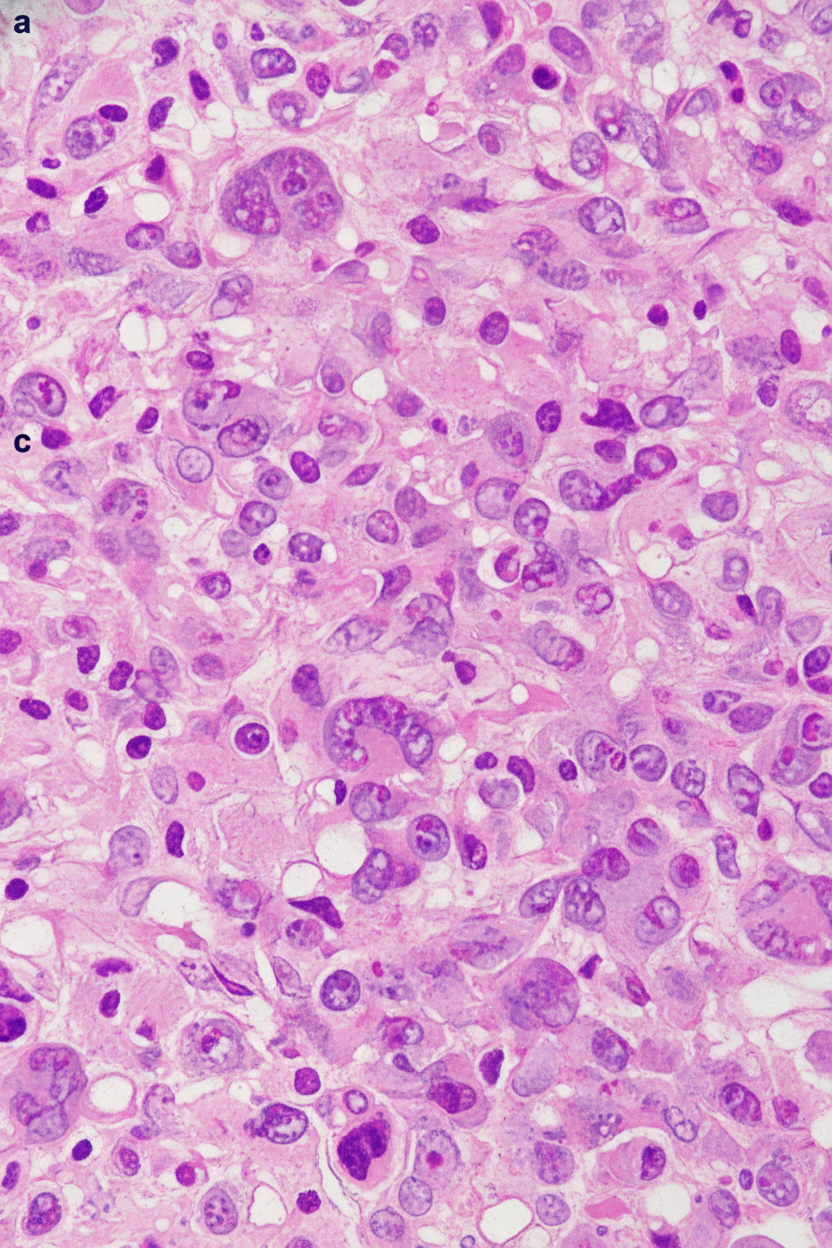
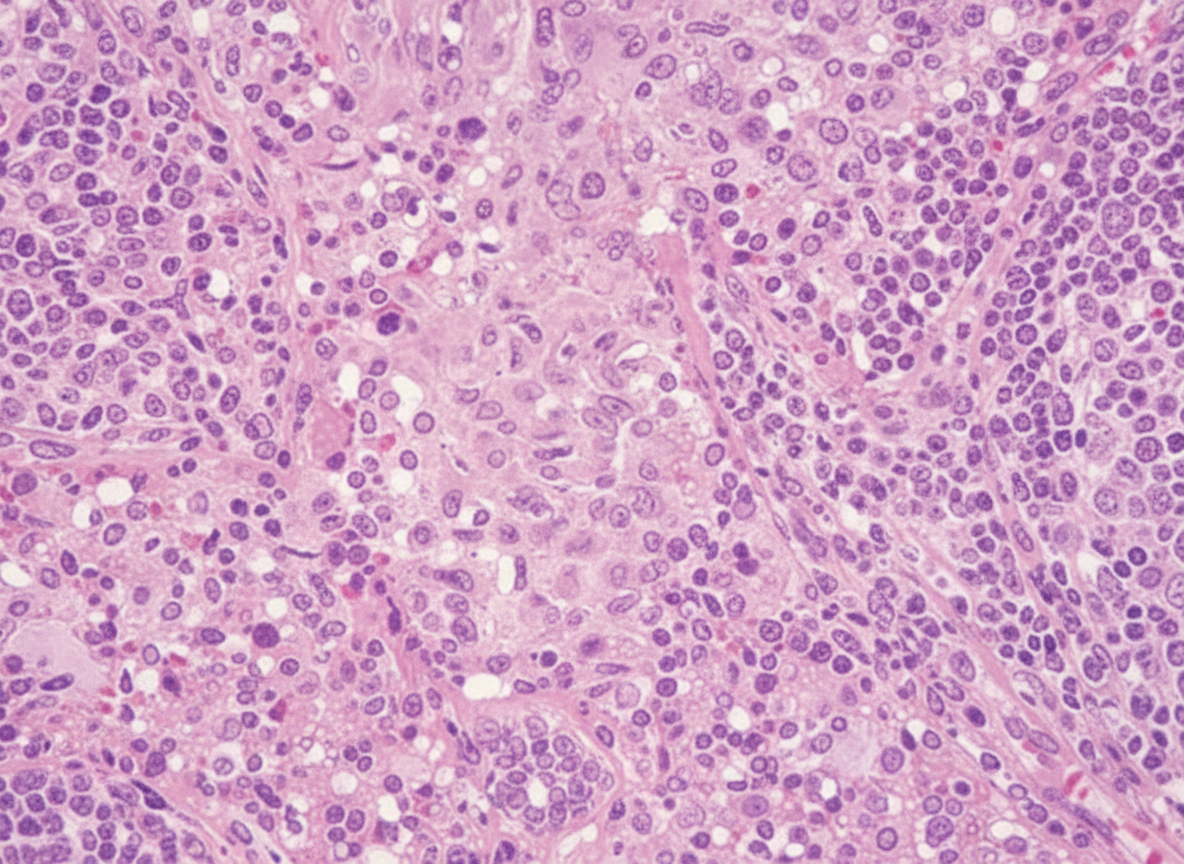
A 45-year-old female has complaints of painless cervical lymphadenopathy with fever and weight loss. A lymph node biopsy was performed. All of the following statements are true regarding this condition except:
Practice by Chapter
Red blood cell disorders
Practice Questions
White blood cell disorders
Practice Questions
Platelet disorders
Practice Questions
Coagulation disorders
Practice Questions
Acute leukemias
Practice Questions
Chronic leukemias
Practice Questions
Myeloproliferative neoplasms
Practice Questions
Myelodysplastic syndromes
Practice Questions
Hodgkin lymphoma
Practice Questions
Non-Hodgkin lymphomas
Practice Questions
Plasma cell disorders
Practice Questions
Bone marrow failure syndromes
Practice Questions
Splenic pathology
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app