
Hematopathology — MCQs

On this page
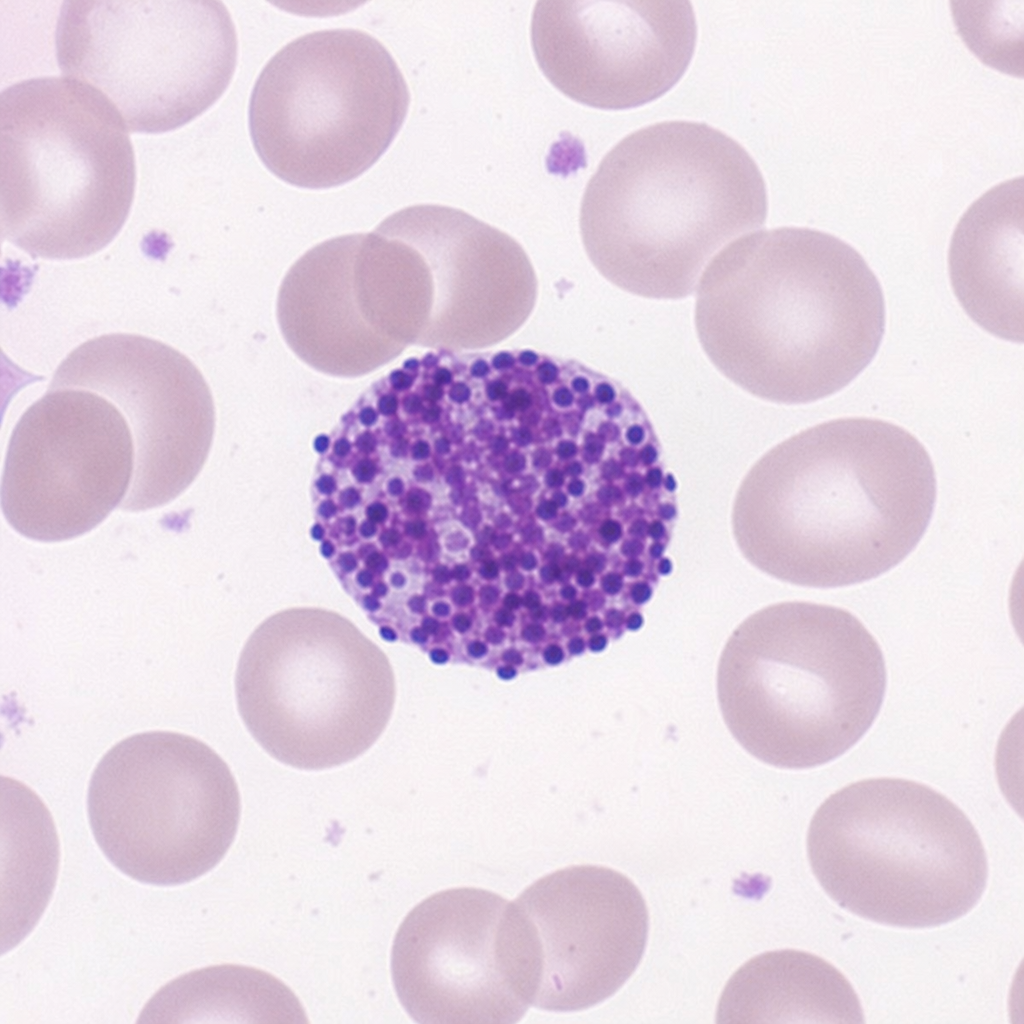
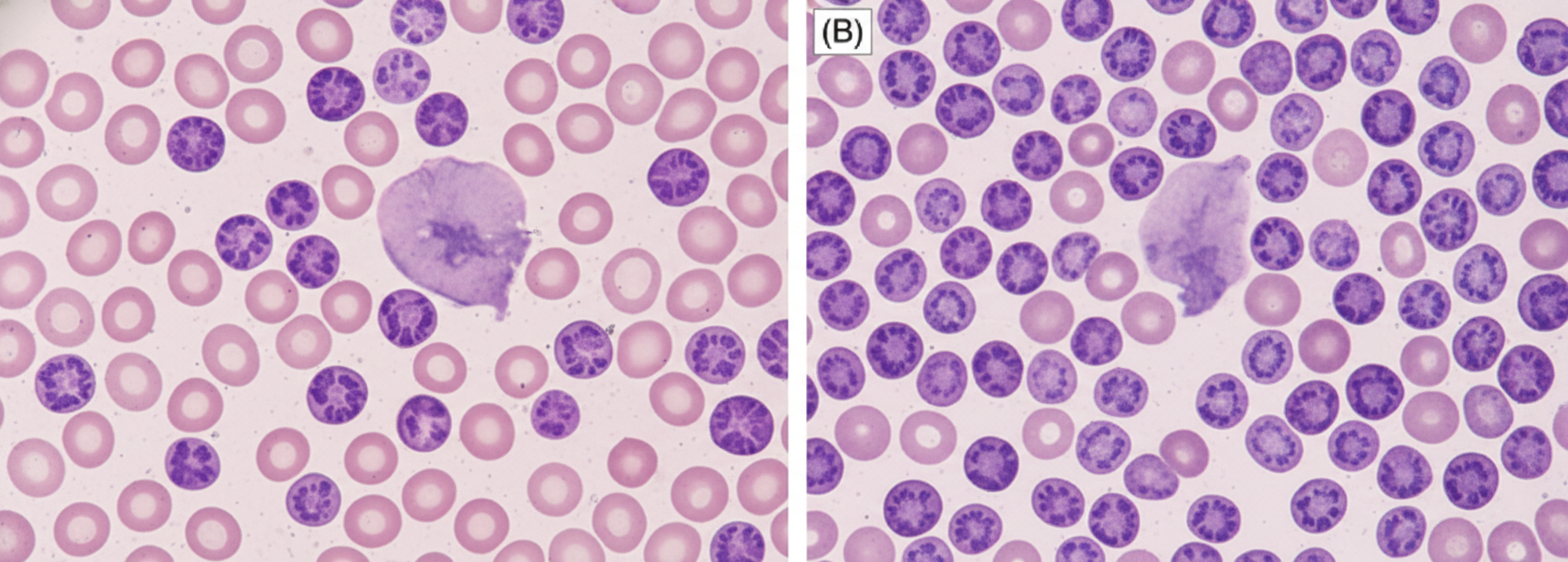
Identify the cell.
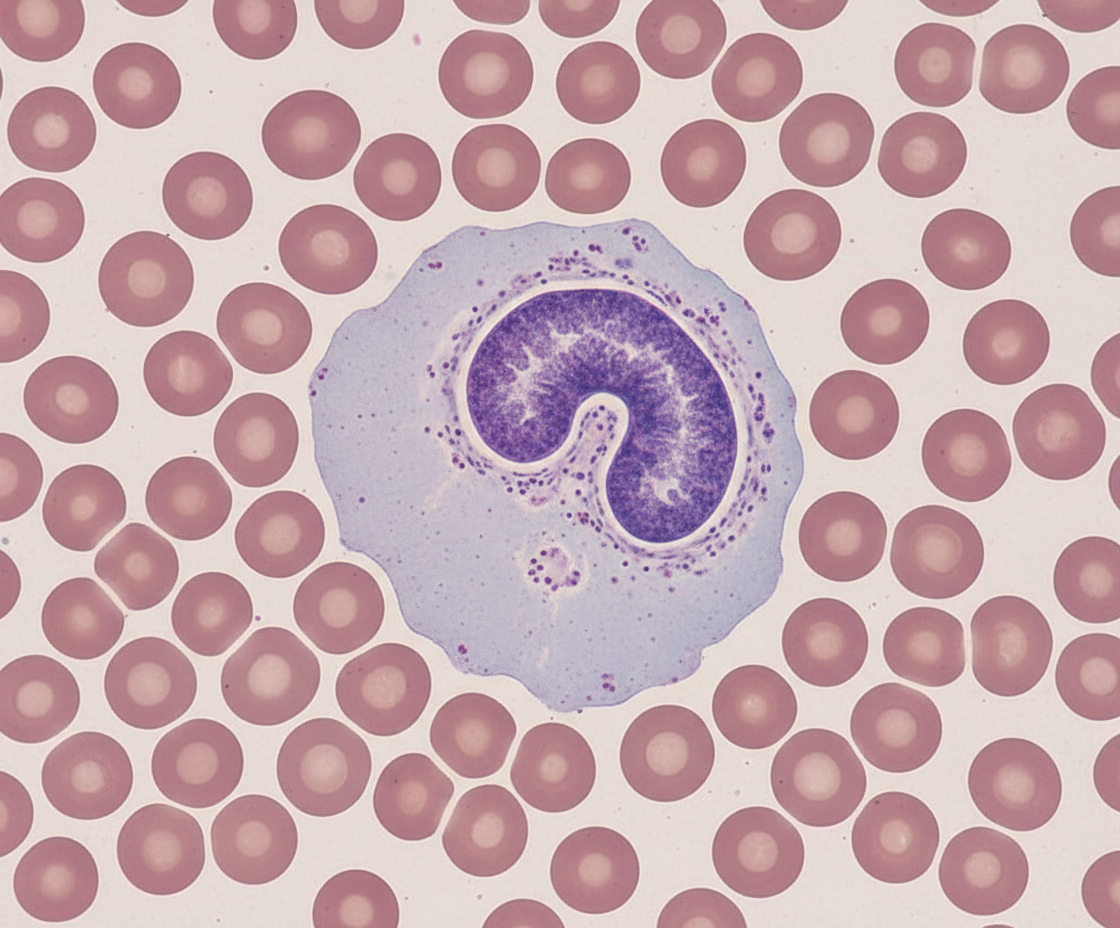
Identify the cell.
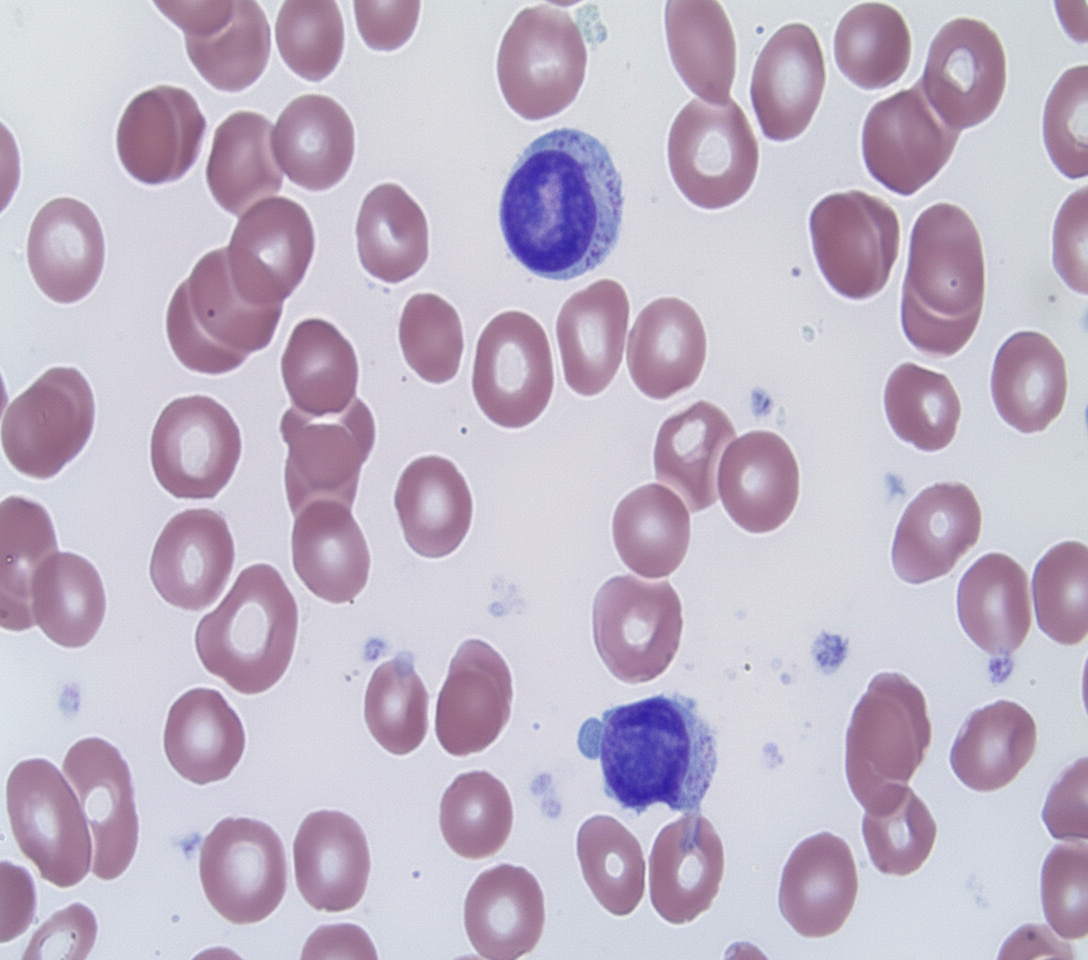
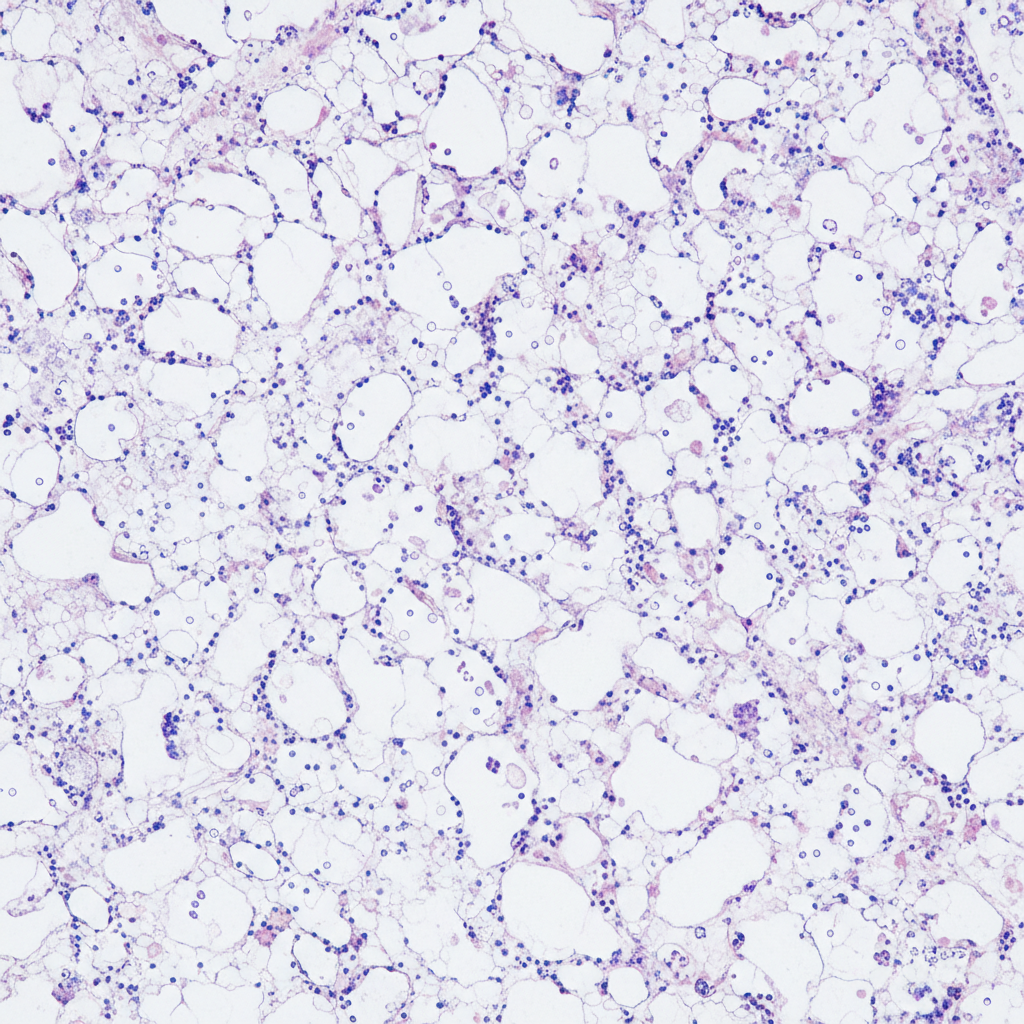
A 65-year-old man presents with pancytopenia and dry tap on bone marrow aspiration. Peripheral smear is given. The diagnosis is:
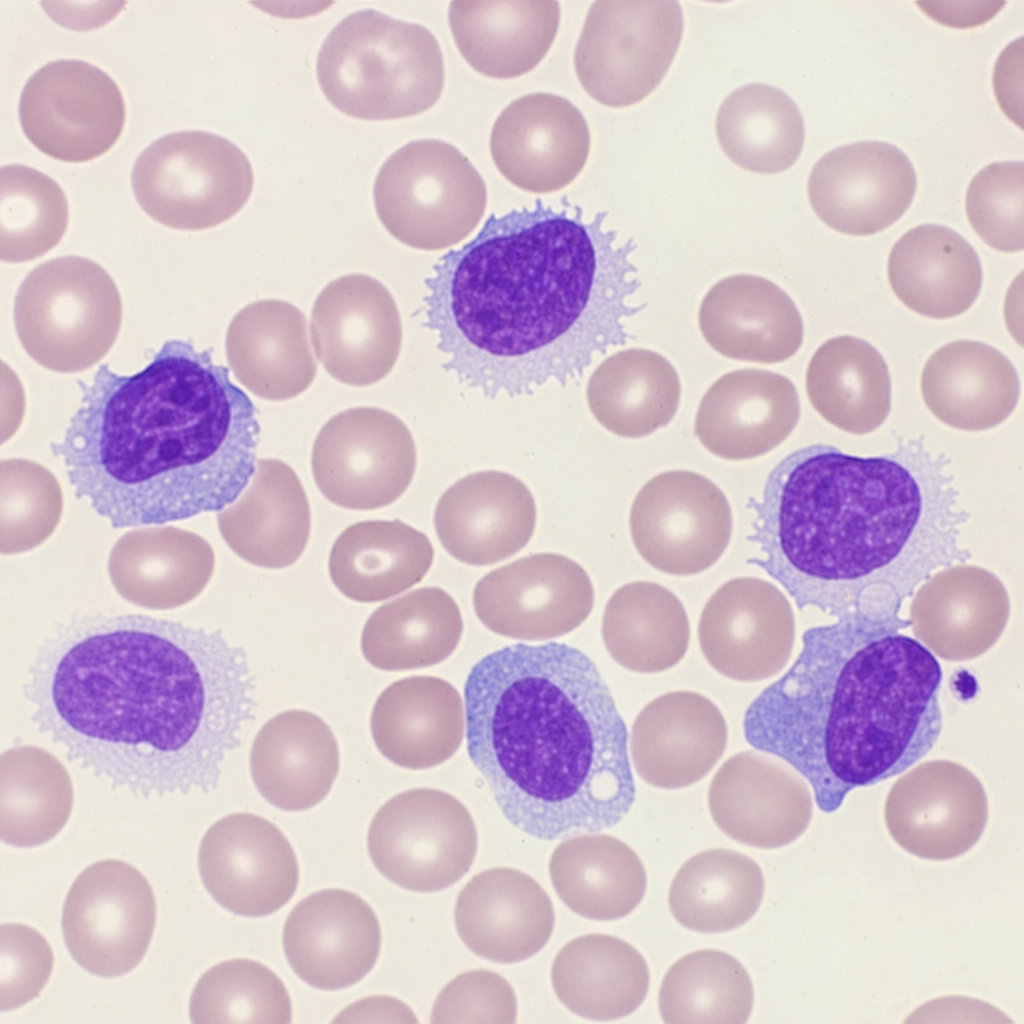
A 15-year-old patient presents with eczematous lesions for last 5 years. On physical examination, the lesions have progressed to present as plaques. Enlarged liver and spleen are noted with increased TLC. The peripheral smear was made. Clinical diagnosis is:
The following bone marrow specimen is suggestive of diagnosis of:
A 70-year-old man presents with painless cervical lymphadenopathy with progressive pallor and petechiae on ankles. The peripheral smear is shown. What is the most likely diagnosis?
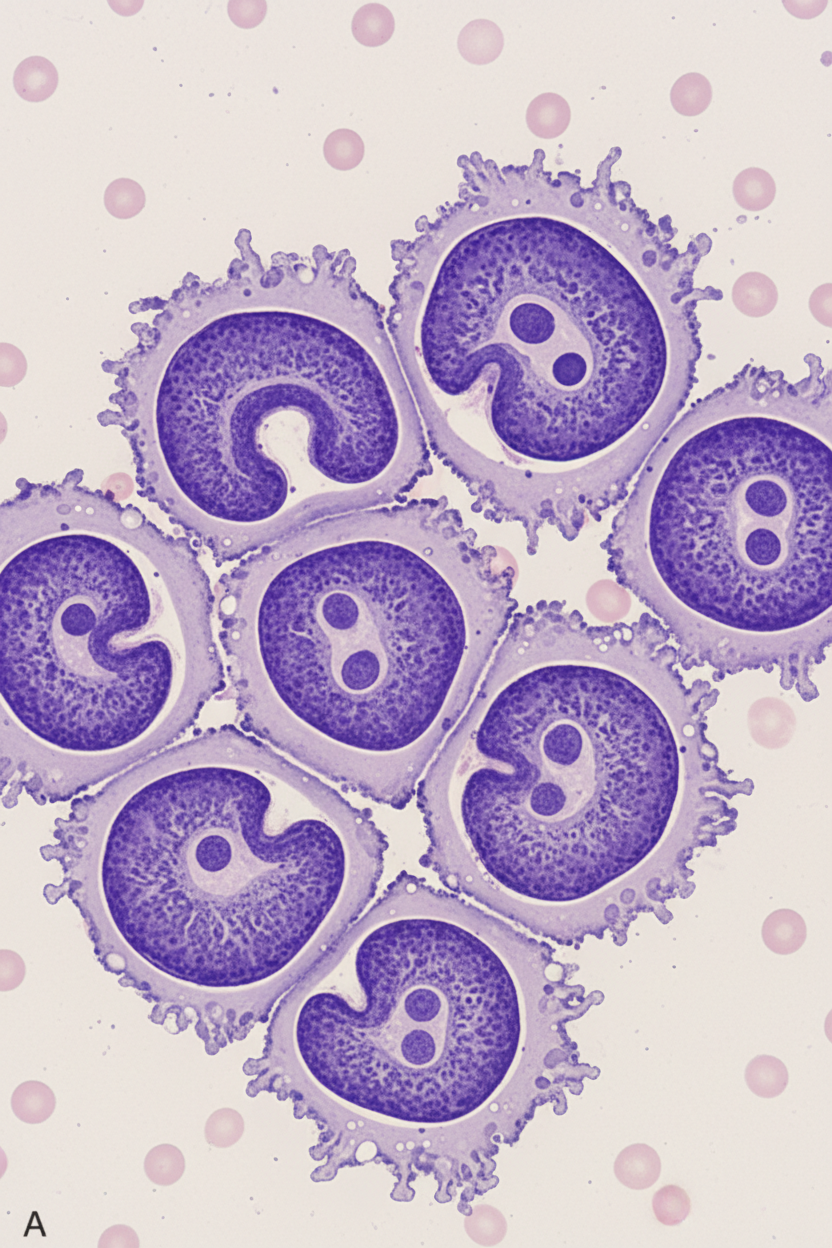
Which is correct about the translocation associated with the neoplasm suggested by these findings in a 25-year-old man who presents with painless cervical lymphadenopathy with progressive pallor and petechiae on ankles. Immunohistochemistry shows nuclear and cytoplasmic ALK staining. Histopathology image is shown below:
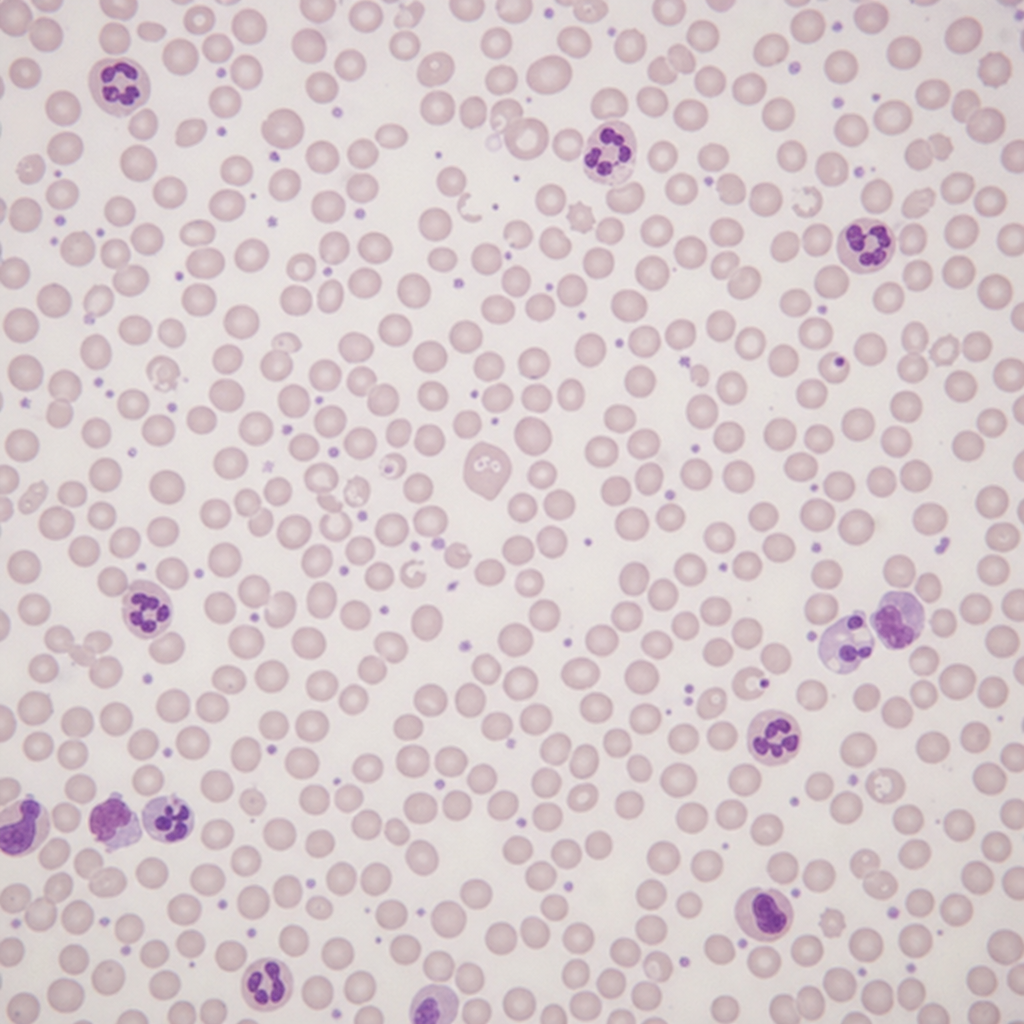
A 25-year-old male presents with acute hemolytic anemia after taking primaquine. His peripheral blood smear shows bite cells and blister cells. The pattern of inheritance of the hematological disorder shown is:
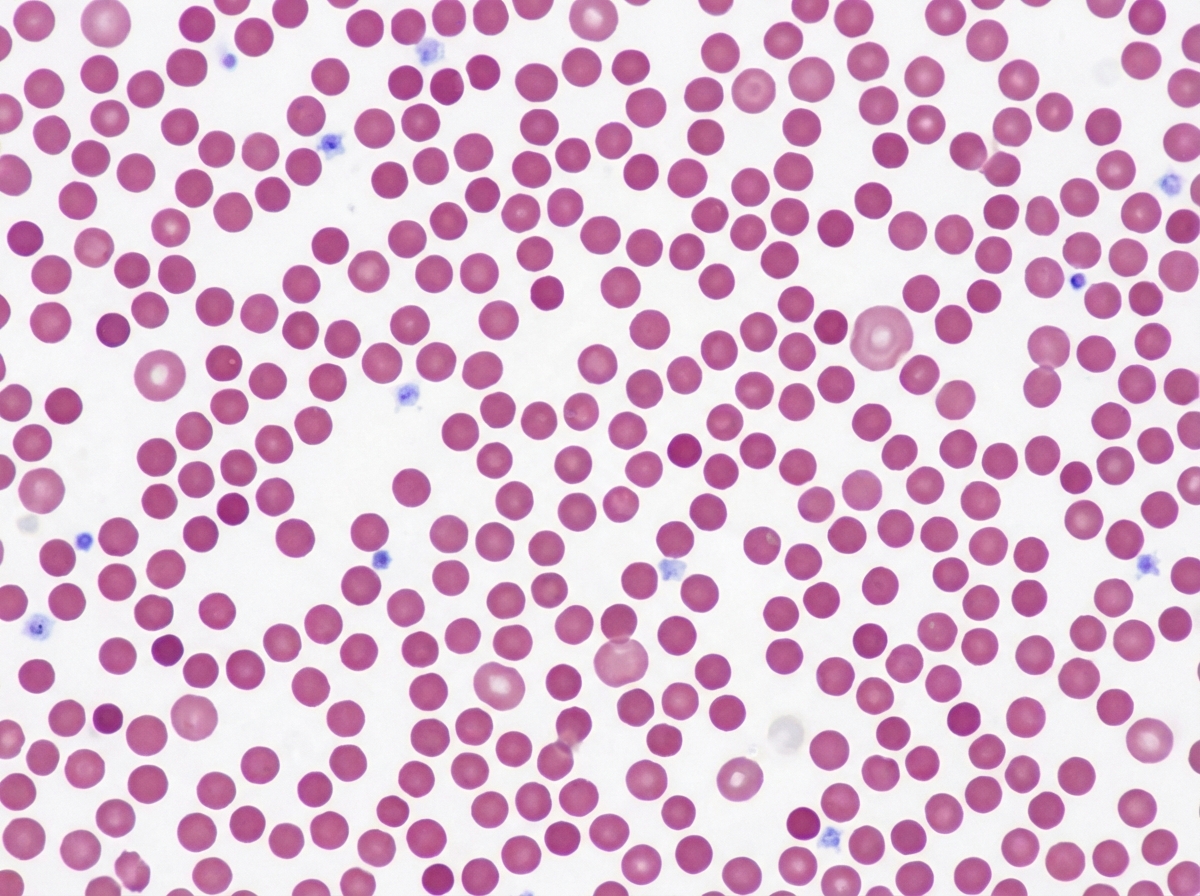
The image shows presence of:
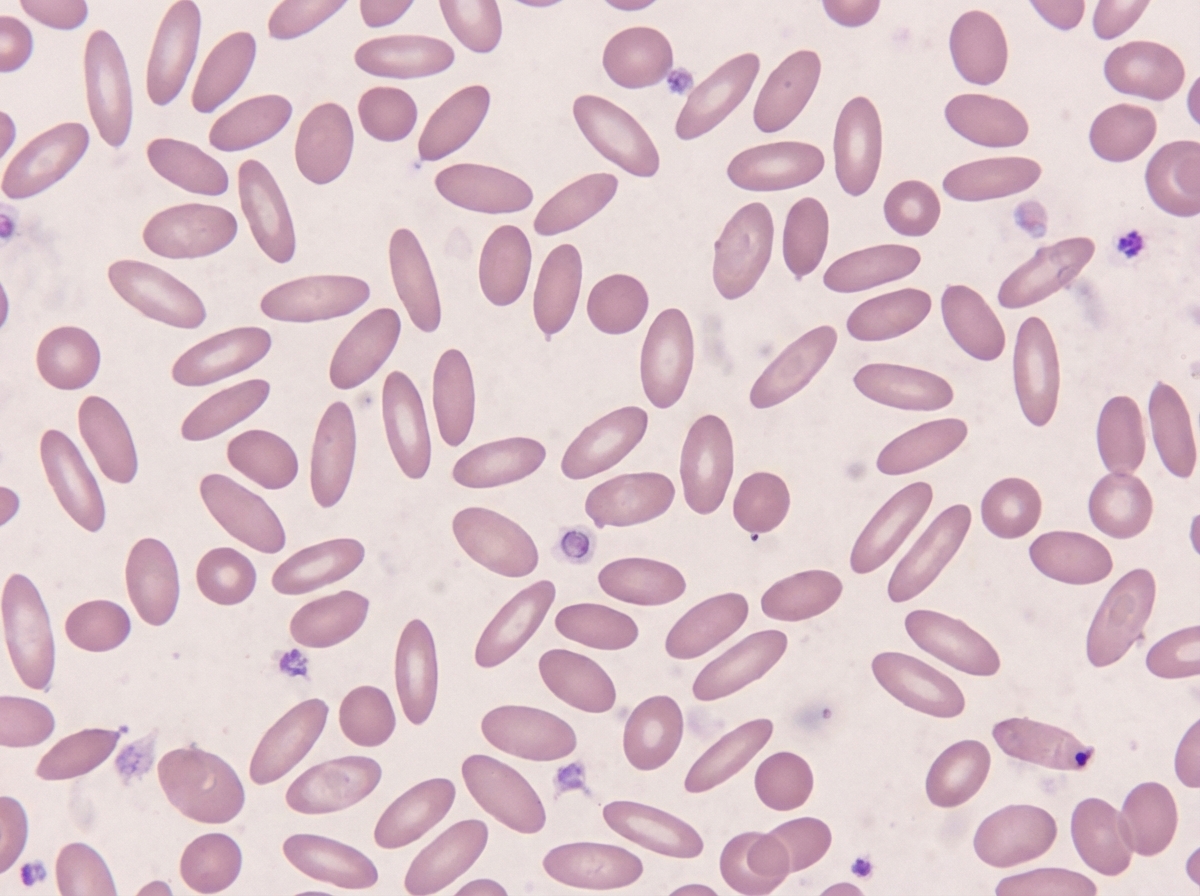
The following image shows presence of:
Practice by Chapter
Red blood cell disorders
Practice Questions
White blood cell disorders
Practice Questions
Platelet disorders
Practice Questions
Coagulation disorders
Practice Questions
Acute leukemias
Practice Questions
Chronic leukemias
Practice Questions
Myeloproliferative neoplasms
Practice Questions
Myelodysplastic syndromes
Practice Questions
Hodgkin lymphoma
Practice Questions
Non-Hodgkin lymphomas
Practice Questions
Plasma cell disorders
Practice Questions
Bone marrow failure syndromes
Practice Questions
Splenic pathology
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app