
Hematopathology — MCQs

On this page
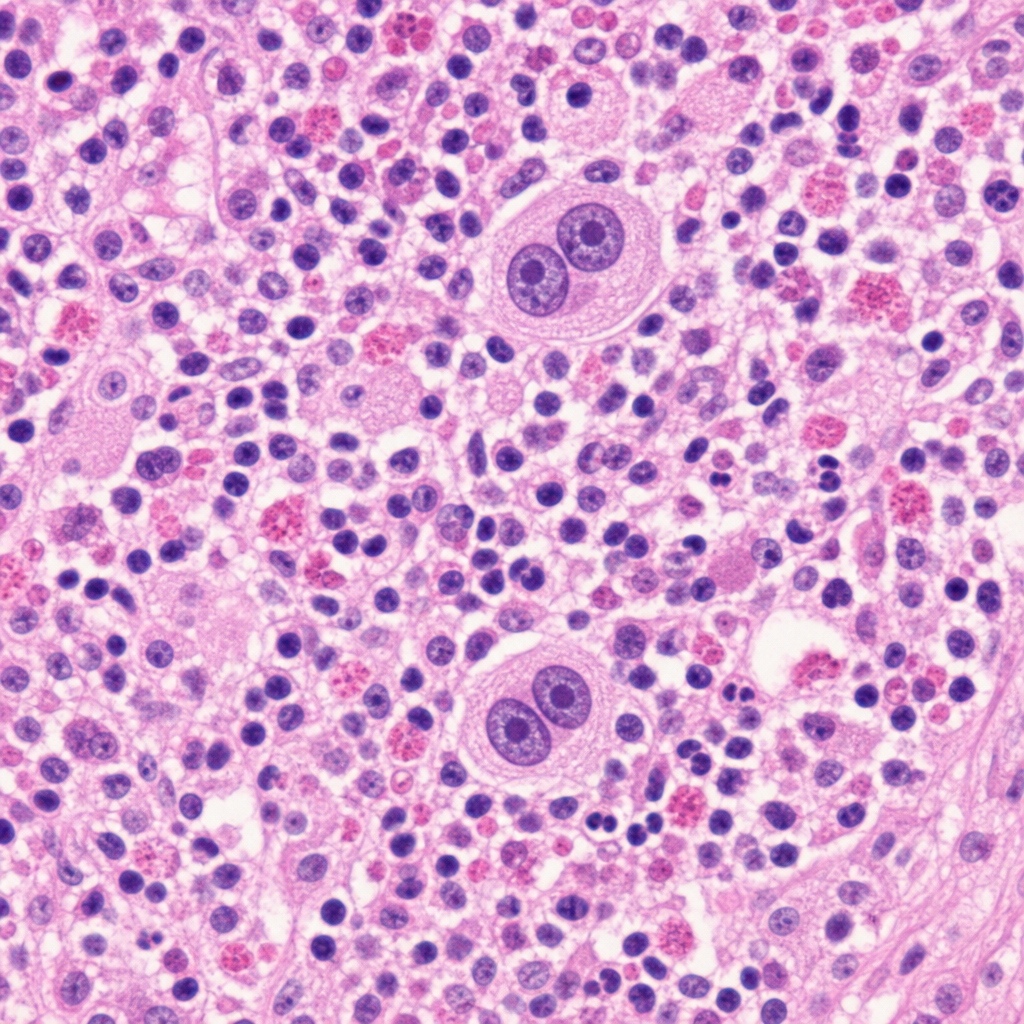
A 34-year-old woman presents with fatigue, night sweats, and a painless right cervical lymph node enlarged to 4 cm over three months. Excisional biopsy is performed. The biopsy demonstrates a diffusely effaced nodal architecture with a mixed inflammatory background of lymphocytes, plasma cells, and eosinophils. Scattered large cells with abundant pale cytoplasm, prominent eosinophilic 'owl-eye' nucleoli, and a mirror-image binucleated morphology are identified. Which of the following cell types is most directly responsible for the characteristic constitutional symptoms in this condition?
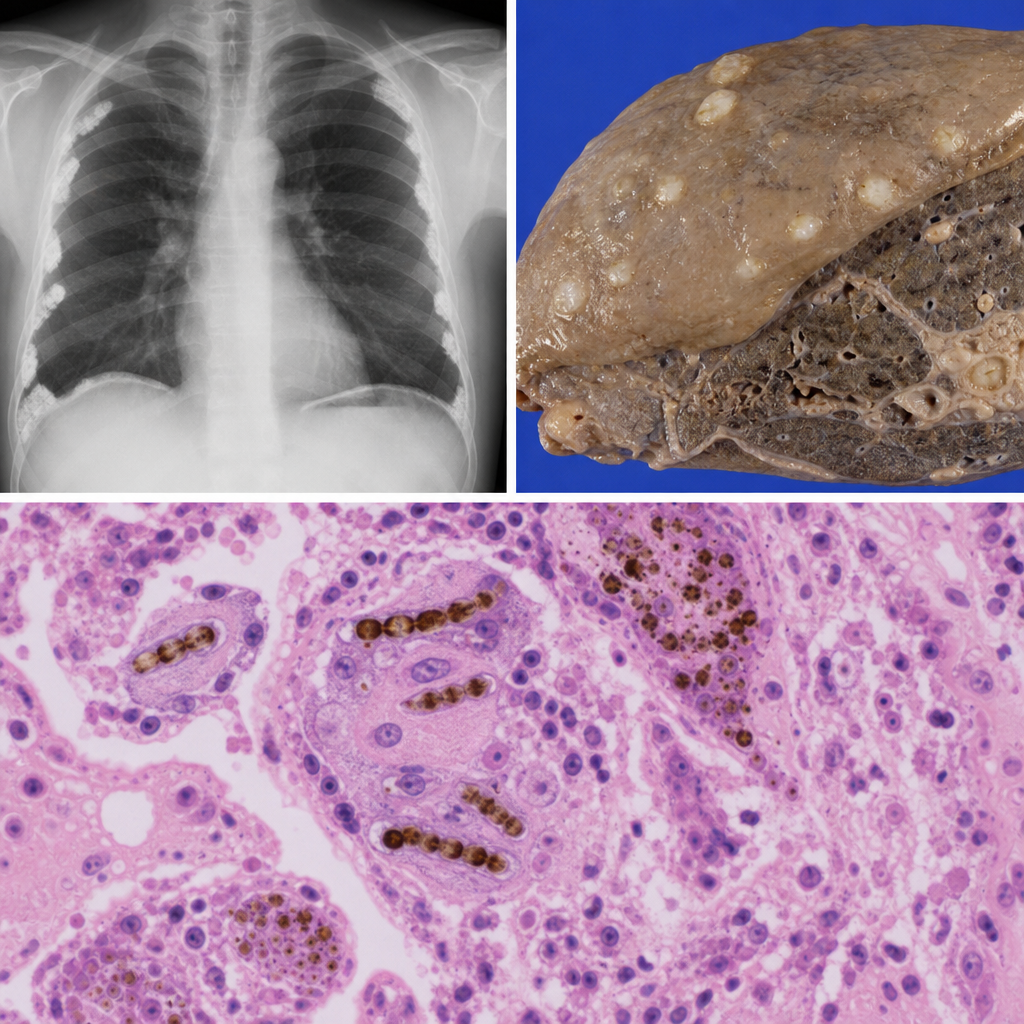
A 58-year-old man with a 40-pack-year smoking history presents with progressive dyspnea and a dry cough. Chest imaging reveals bilateral pleural plaques. A pleural biopsy is performed. Histological examination reveals elongated beaded structures with a golden-brown segmented coating within macrophages and lung parenchyma. Which of the following best describes the pathological significance of this finding?
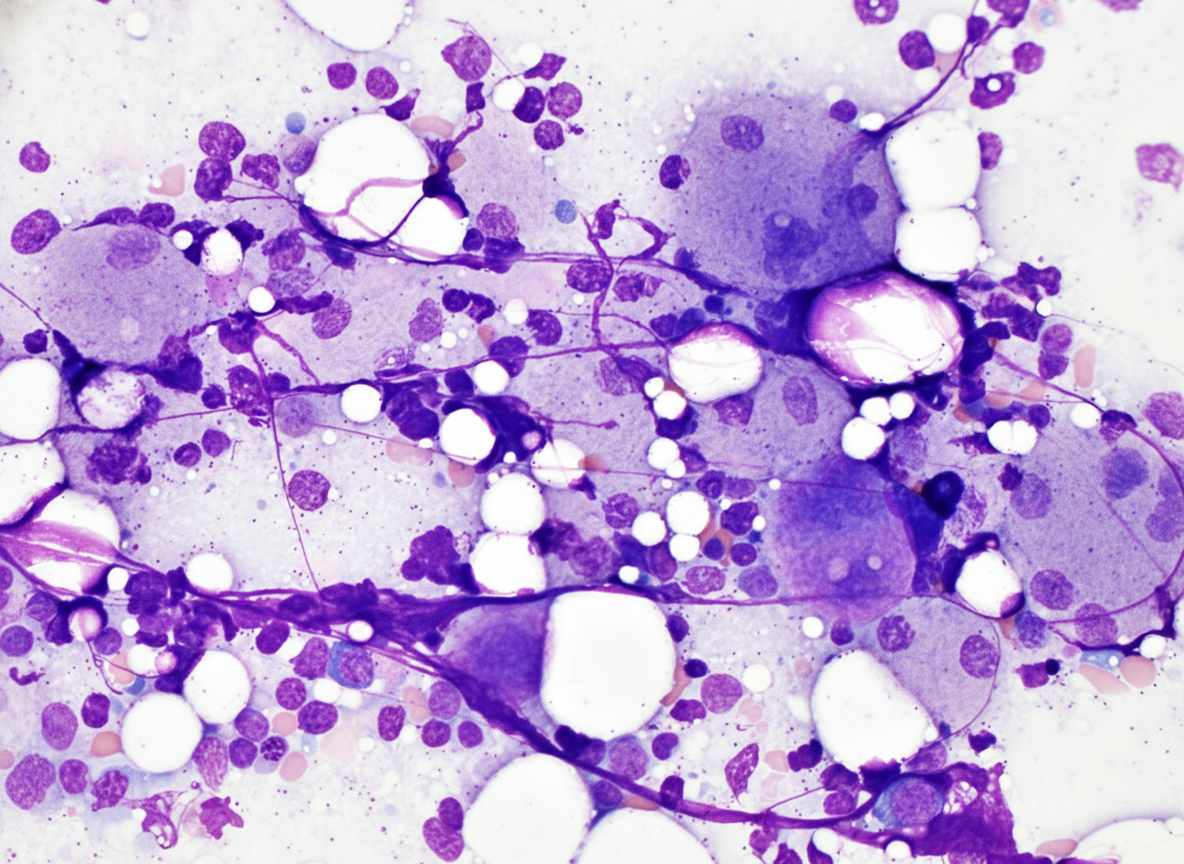
Infant with anemia, poor growth and bleeding from nose was brought to emergency. On examination hepatosplenomegaly was noted, and serum chitotriosidase levels are elevated. Bone marrow examination was done. Diagnosis is:
The vacutainer shown below is used for collecting sample for? (AIIMS Nov 2017)

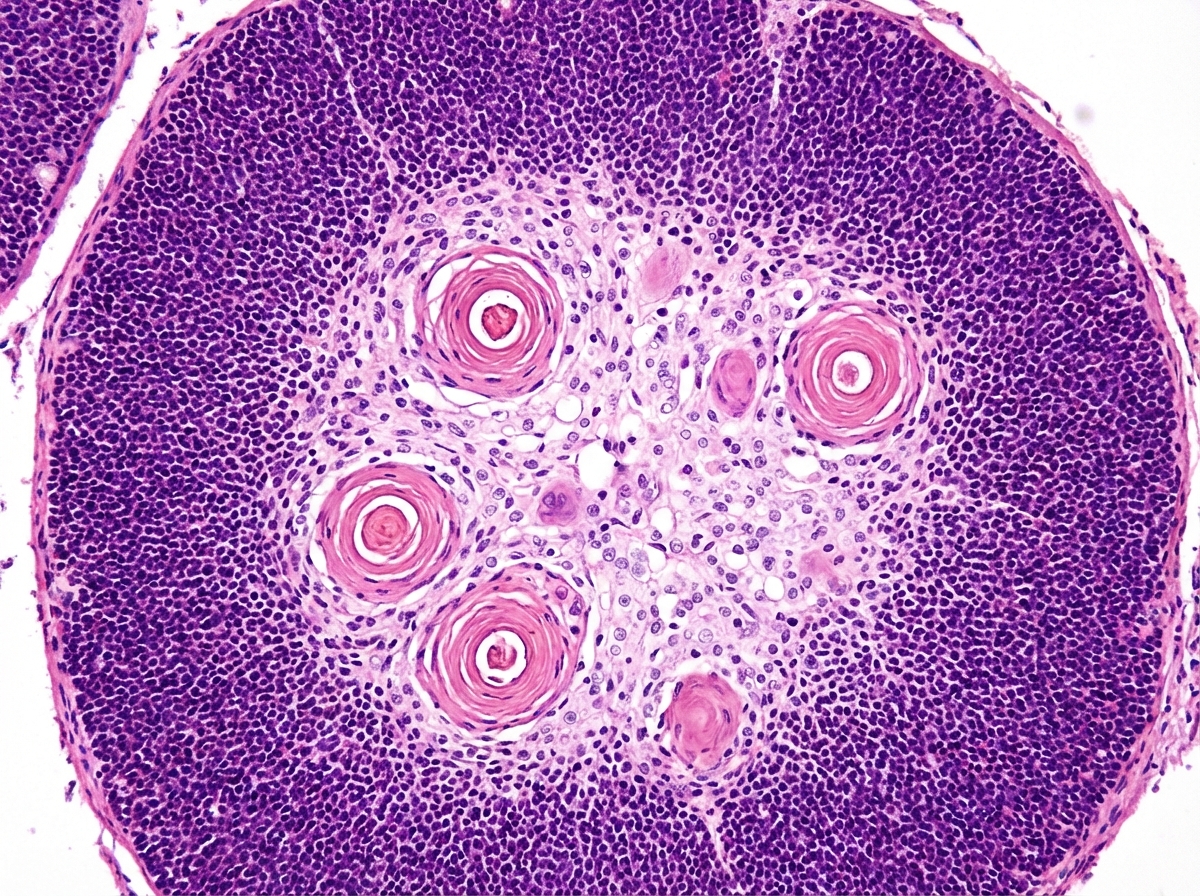
Identify the tissue:
Practice by Chapter
Red blood cell disorders
Practice Questions
White blood cell disorders
Practice Questions
Platelet disorders
Practice Questions
Coagulation disorders
Practice Questions
Acute leukemias
Practice Questions
Chronic leukemias
Practice Questions
Myeloproliferative neoplasms
Practice Questions
Myelodysplastic syndromes
Practice Questions
Hodgkin lymphoma
Practice Questions
Non-Hodgkin lymphomas
Practice Questions
Plasma cell disorders
Practice Questions
Bone marrow failure syndromes
Practice Questions
Splenic pathology
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app