
GI — MCQs

On this page
A 52-year-old man presents with 2 months of diarrhea, abdominal pain, and fatigue. He reports a weight loss of 4 kg (8 lb). He also says his joints have been hurting recently, as well. Past medical history is unremarkable. Review of systems is significant for problems with concentration and memory. Physical examination is unremarkable. A GI endoscopy is performed with a biopsy of the small bowel. Which of the following histologic finding would most likely be seen in this patient?
A 22-year-old Caucasian female presents with severe right lower quadrant pain, malaise, and diarrhea. The physician performs an endoscopy and finds disease involvement in the terminal ileum, noting that the disease process is patchy with normal intervening mucosa. The entire wall of the region is thickened and inflamed, which may directly lead to formation of:
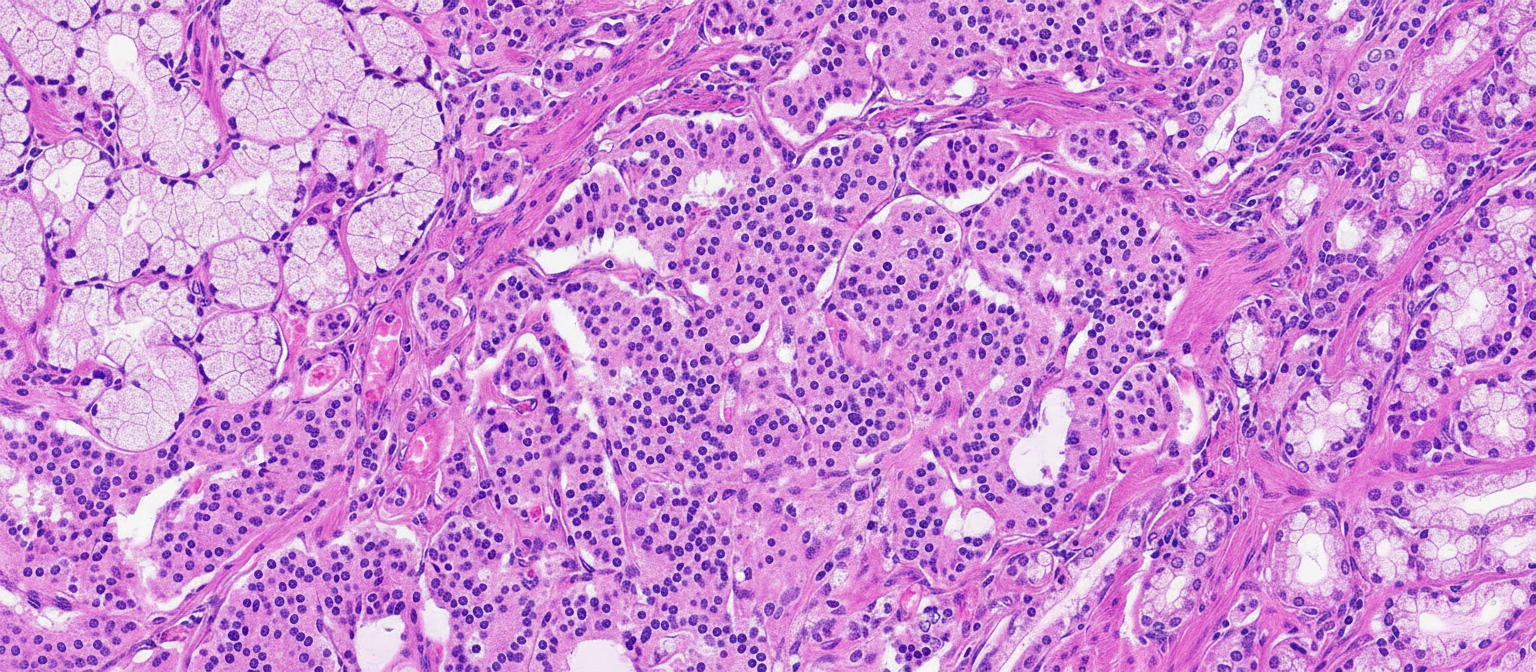
A previously healthy 67-year-old man comes to the physician because of a history of recurrent right lower abdominal pain for the past 2 years. A CT scan shows a 1.2-cm (0.47-in) mass located in the terminal ileum. He undergoes surgical removal of the mass. A photomicrograph of the resected specimen is shown. Cells from this tissue are most likely to stain positive for which of the following?
An otherwise healthy 56-year-old man comes to the physician for a 2-year history of recurrent upper abdominal pain and fullness that worsens after meals. Urea breath test is positive. An endoscopy shows diffuse mucosal atrophy and patchy erythema, but no ulcer. A biopsy from which of the following areas is most likely to yield an accurate diagnosis?
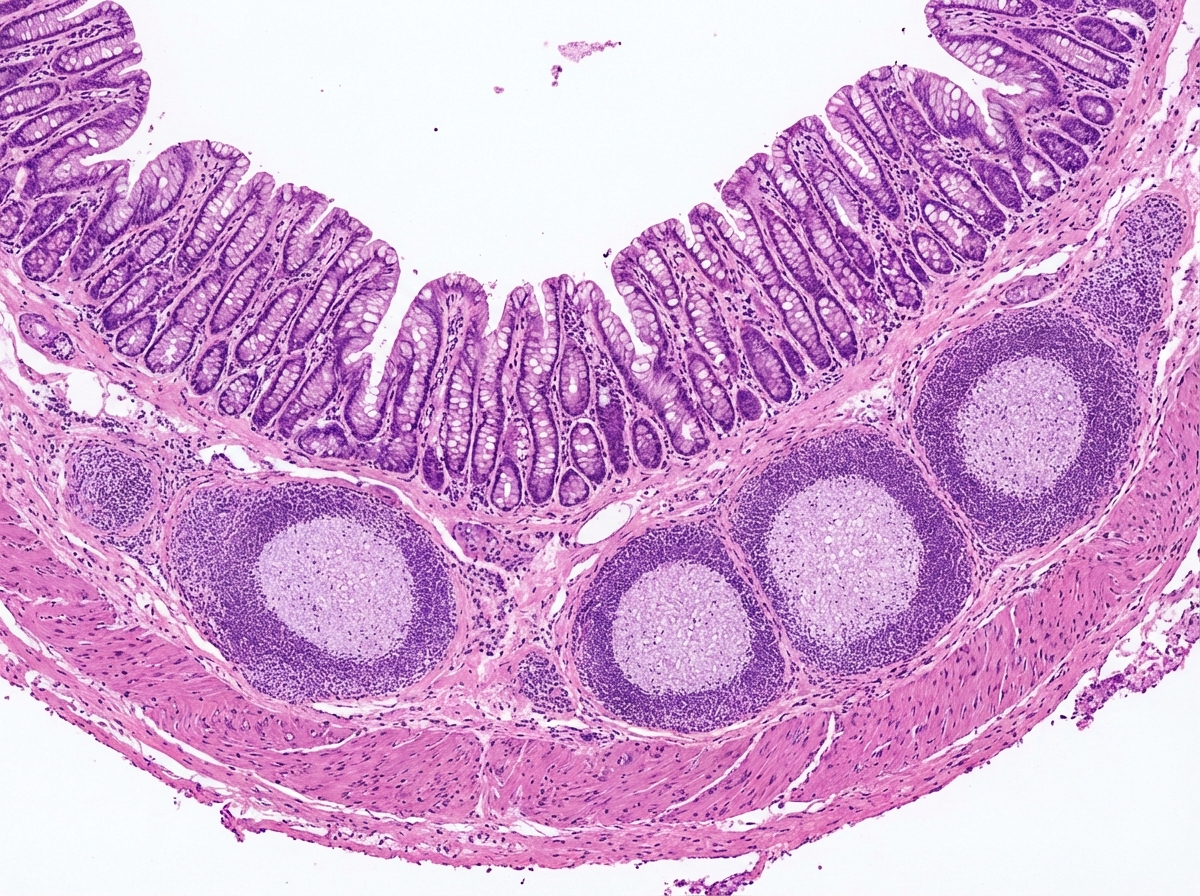
A 13-year-old boy presents to the emergency department with severe right-lower-quadrant abdominal pain. Workup reveals acute appendicitis, and he subsequently undergoes laparoscopic appendectomy. The appendix is sent for histological examination. A pathologist reviews the slide shown in the image below. Which statement about the structures marked within the yellow circles is correct?
A 13-year-old boy is brought to the pediatrician by his parents who are concerned about his short stature. He also has had recurrent episodes of diarrhea. Past medical history is significant for iron deficiency anemia diagnosed 6 months ago. Physical examination is unremarkable except that he is in the 9th percentile for height. Serum anti-tissue transglutaminase (anti-tTG) antibodies are positive. An upper endoscopy along with small bowel luminal biopsy is performed. Which of the following histopathologic changes would most likely be present in the mucosa of the duodenal biopsy in this patient?
A 75-year-old man comes to his primary care physician because he has been having diarrhea and difficulty breathing. The diarrhea has been intermittent with frequent watery stools that occur along with abdominal cramps. Furthermore, the skin on his face and upper chest feels hot and changes color in episodes lasting from a few minutes to hours. Finally, the patient complains of loss of appetite and says that he has unexpectedly lost 20 pounds over the last two months. Based on clinical suspicion, magnetic resonance imaging is obtained showing a small mass in this patient's lungs. Which of the following is associated with the most likely cause of this patient's symptoms?
A 47-year-old presents to the clinic with a 3-day history of severe mid-epigastric abdominal pain radiating to the back. The patient has hypertension, diabetes mellitus, and hypertriglyceridemia. Prescription medications include enalapril, metformin, sitagliptin, glargine, lispro, and fenofibrate. The patient has not had a cigarette in more than 35 years, and reports only having 1 or 2 drinks during special occasions such as weddings and family reunions. The blood pressure is 146/90 mm Hg, the heart rate is 88/min, the respiratory rate is 10/min, and the temperature is 37.8°C (100.0°F). On physical examination, the patient appears uncomfortable but alert. The visualization of the sclera is negative for jaundice. The neck is supple and non-tender without nodules. There are no heart murmurs. The lungs are clear to auscultation bilaterally. The palpation of the abdomen elicits pain in the epigastric region. The liver is palpable along the costal margin, and the Murphy's sign is negative. The laboratory results are as follows: Na+ 138 mEq/L K+ 4.2 mEq/L Cl- 108 mmol/L HCO-3 20 mmol/L BUN 18 mg/dL Cr 1.0 mg/dL Glucose 154 mg/dL LDL 117 mg/dL HDL 48 mg/dL TG 942 mg/dL AST 45 IU/L ALT 48 IU/L GGT 27 IU/L Amylase 110 U/L Lipase 250 U/L According to the clinical vignette, which of the following is the most likely diagnosis of the patient?
A 40-year-old man presents to his primary care provider complaining of abdominal pain. The patient reports a dull pain that has been present for 4 weeks now. The patient states that the pain is located to his right upper quadrant and does not change with eating. The patient denies any alcohol or illicit substance use, stating that he is meticulous about eating healthy since he is a professional bodybuilder. The patient reports no history of malignancy. On exam, the patient's temperature is 98.2°F (36.8°C), blood pressure is 130/86 mmHg, pulse is 60/min, and respirations are 12/min. The patient has an athletic build, and his exam is unremarkable for any palpable mass or abdominal tenderness. On further questioning, the patient does endorse a 5-year history of using anabolic steroids for bodybuilding. Imaging demonstrates an enhancing liver nodule. Which of the following is the most likely histopathologic finding of this patient’s disease?
A 13-year-old African American boy with sickle cell disease is brought to the emergency department with complaints of abdominal pain over the last 24 hours. The pain is situated in the right upper quadrant and is sharp in nature with a score of 8/10 and radiates to tip of the right scapula. He also complains of anorexia and nausea over the past 2 days. He has been admitted into the hospital several times for pain episodes involving his legs, hands, thighs, lower back, and abdomen. His last hospital admission was 4 months ago for acute chest pain, and he was treated with antibiotics, analgesics, and intravenous fluid. He takes hydroxyurea with occasional red blood cell exchange. Both of his parents are in good health. Temperature is 38°C (100.4°F), blood pressure is 133/88 mm Hg, pulse is 102/min, respiratory rate is 20/min, and BMI is 18 kg/m2. On examination, he is in pain with a tender abdomen with painful inspiration. Soft palpation of the right upper quadrant causes the patient to cry out in pain. Laboratory test Complete blood count Hemoglobin 8.5 g/dL MCV 82 fl Leukocytes 13,500/mm3 Platelets 145,000/mm3 Basic metabolic panel Serum Na+ 135 mEq/L Serum K+ 3.9 mEq/L Serum Cl- 101 mEq/L Serum HCO3- 23 mEq/L Liver function test Serum bilirubin 2.8 mg/dL Direct bilirubin 0.8 mg/dL AST 30 U/L ALT 35 U/L Serum haptoglobin 23 mg/dL (41–165 mg/dL) Ultrasonography of abdomen shows the following image. What is the pathogenesis of this ultrasound finding?

Practice by Chapter
Esophageal pathology
Practice Questions
Gastritis and peptic ulcer disease
Practice Questions
Gastric tumors
Practice Questions
Malabsorption syndromes
Practice Questions
Inflammatory bowel diseases
Practice Questions
Intestinal infections
Practice Questions
Diverticular disease
Practice Questions
Vascular disorders of bowel
Practice Questions
Colon polyps and neoplasms
Practice Questions
Appendicitis
Practice Questions
Peritonitis
Practice Questions
Hernia complications
Practice Questions
Gastrointestinal stromal tumors
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app