
GI — MCQs

On this page
A 56-year-old man comes to the physician because of intermittent retrosternal chest pain. Physical examination shows no abnormalities. Endoscopy shows salmon pink mucosa extending 5 cm proximal to the gastroesophageal junction. Biopsy specimens from the distal esophagus show nonciliated columnar epithelium with numerous goblet cells. Which of the following is the most likely cause of this patient's condition?
A 34-year-old man with worsening refractory epigastric pain secondary to long-standing gastroesophageal reflux disease presents for endoscopic evaluation. Past medical history is also significant for type 2 diabetes mellitus that was diagnosed 3 years ago, managed medically. Current medications are metformin, metoclopramide, and omeprazole. Which of the following best describes this patient’s most likely endoscopic findings?
A 47-year-old man presents with daily substernal chest pain for the past year. In addition, he says that he often suffers from hoarseness and a cough in the mornings. His wife has also reported that he has developed bad breath. Past medical history is significant for diabetes mellitus, managed with metformin. His physical examination is unremarkable. ECG is normal. An esophagogastroduodenoscopy is performed. The lower third of the esophagus appears erythematous, and a biopsy of the gastroesophageal junction is taken. When he is given sublingual nitroglycerin, it is noted that his chest discomfort is worsened. Which of the following would be expected in this patient’s biopsy?
A 41-year-old male who takes NSAIDs regularly for his chronic back pain develops severe abdominal pain worse with eating. Upper endoscopy is performed and the medical student asks the supervising physician how the histological differentiation between a gastric ulcer and erosion is made. Which of the following layers of the gastric mucosa MUST be breached for a lesion to be considered an ulcer?
A 49-year-old woman is admitted to the hospital for the evaluation of postprandial colicky pain in the right upper quadrant of the abdomen. Abdominal ultrasound shows multiple round, hyperechoic structures within the gallbladder lumen. She undergoes a cholecystectomy. A photograph of the content of her gallbladder is shown. This patient is most likely to have which of the following additional conditions?

A 22-year-old man comes to the physician because of a 3-week history of abdominal pain, loose, non-bloody stools, and intermittent nausea. He also reports intermittent fever. He has not had vomiting, tenesmus, or rectal pain. He has no history of serious illness and takes no medications. His vital signs are within normal limits. Rectal exam is unremarkable. Laboratory studies show a leukocyte count of 15,200/mm3 and an erythrocyte sedimentation rate of 44 mm/h. Test of the stool for occult blood and stool studies for infection are negative. A CT scan of the abdomen shows mural thickening and surrounding fat stranding of discrete regions of the terminal ileum and transverse colon. A colonoscopy is performed and biopsy specimens of the affected areas of the colon are taken. Which of the following findings is most specific for this patient's most likely diagnosis?
A 22-year-old woman presents to the emergency department with a 3-day history of fever and abdominal pain. She says that the pain is located in the left lower quadrant of the abdomen and feels crampy in nature. The pain has been associated with bloody diarrhea and joint tenderness. She has no past medical history but says that she returned 2 weeks ago from vacation in Asia where she tried many new foods. Her family history is significant for multiple cancers in close relatives. Physical exam reveals swollen ulcers on her legs, and colonoscopy reveals contiguous ulcerations from the rectum through the descending colon. Which of the following is associated with the most likely cause of this patient's symptoms?
A 45-year-old man comes to the physician for his routine health maintenance examination. He was diagnosed with diabetes mellitus 4 years ago. His medical history is otherwise unremarkable. He takes no medications other than daily metformin. He has consumed a can of beer every night for the past 10 years. His blood pressure is 145/90 mm Hg. His body mass index is 31 kg/m2. Physical examination shows no abnormalities. Laboratory studies show: Partial thromboplastin time (activated) 30 seconds (N=25-40 seconds) Prothrombin time 13 seconds (N=11-15 seconds) International normalized ratio 1.2 Serum albumin 4 g/dL Bilirubin, total 0.9 mg/dL Direct 0.2 mg/dL Alkaline phosphatase 45 U/L Aspartate aminotransferase (AST, GOT) 43 U/L Alanine aminotransferase (ALT, GPT) 56 U/L γ-Glutamyltransferase (GGT) 43 U/L (N=5-50 U/L) Hepatitis A antibody Negative Hepatitis B surface antigen Negative Hepatitis C antibody Negative Liver biopsy shows excessive intracellular fat accumulation, hepatocyte ballooning, and perivenular infiltration of lymphocytes and neutrophils without significant fibrosis. Which of the following best describes these findings?
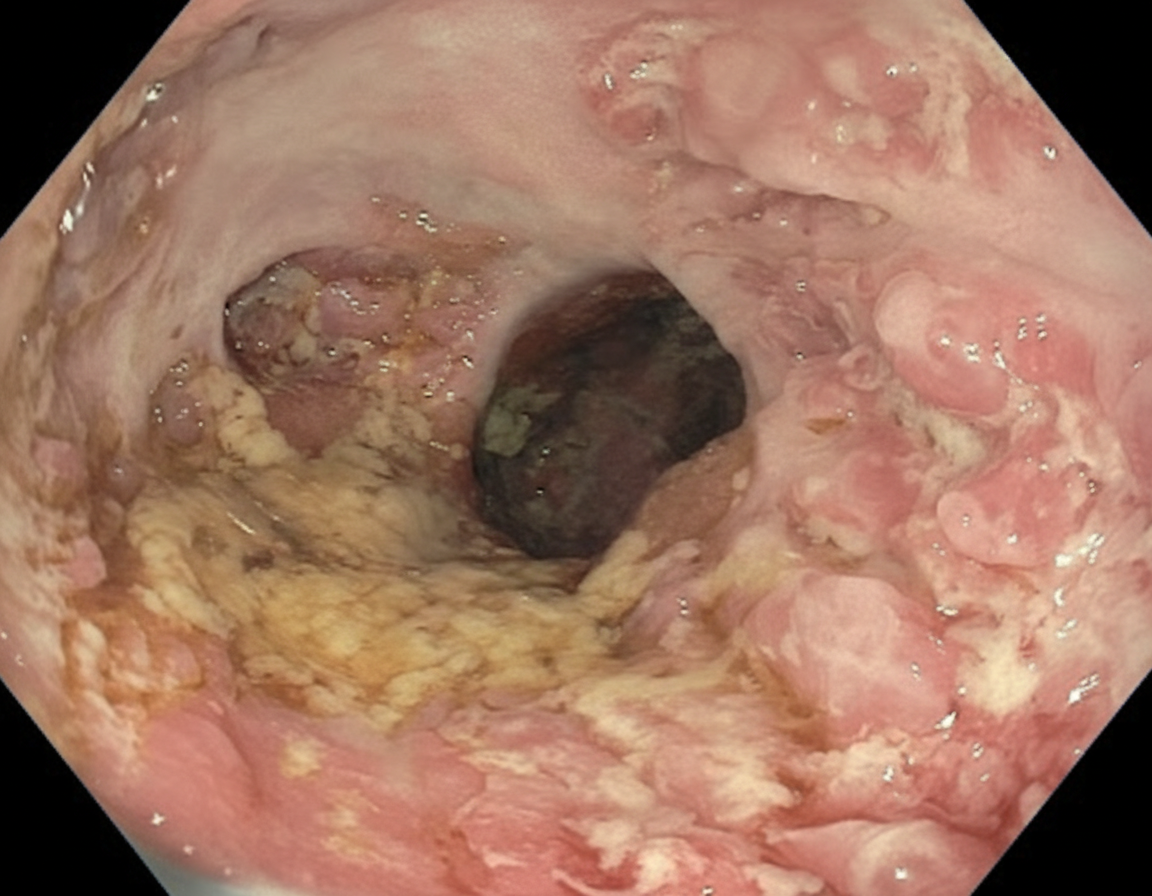
A 28-year-old man comes to the physician because of a 6-month history of progressive fatigue and intermittent diarrhea. During this time, he has had a 6-kg (13-lb) weight loss. Physical examination shows pale conjunctivae. Abdominal examination shows tenderness to palpation in the lower quadrants. A colonoscopy is performed and shows inflammation extending continuously proximally from the rectum without skip lesions; an image from the descending colon is shown. Further evaluation is most likely to show which of the following findings?
A 35-year-old Caucasian female presents with anemia, malaise, bloating, and diarrhea. Past genetic testing revealed that this patient carries the HLA-DQ2 allele. The physician suspects that the patient's presentation is dietary in cause. Which of the following findings would definitively confirm this diagnosis?
Practice by Chapter
Esophageal pathology
Practice Questions
Gastritis and peptic ulcer disease
Practice Questions
Gastric tumors
Practice Questions
Malabsorption syndromes
Practice Questions
Inflammatory bowel diseases
Practice Questions
Intestinal infections
Practice Questions
Diverticular disease
Practice Questions
Vascular disorders of bowel
Practice Questions
Colon polyps and neoplasms
Practice Questions
Appendicitis
Practice Questions
Peritonitis
Practice Questions
Hernia complications
Practice Questions
Gastrointestinal stromal tumors
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app