
GI — MCQs

On this page
A previously healthy 35-year-old woman comes to the physician for a 3-week history of alternating constipation and diarrhea with blood in her stool. She has not had any fevers or weight loss. Her father died of gastric cancer at 50 years of age. Physical examination shows blue-gray macules on the lips and palms of both hands. Colonoscopy shows multiple polyps throughout the small bowel and colon with one ulcerated polyp at the level of the sigmoid colon. Multiple biopsy specimens are collected. These polyps are most likely to be characterized as which of the following histological subtypes?
A 27-year-old woman presents to her primary care physician for evaluation of involuntary weight loss and recurrent abdominal pain. She noticed blood in her stool several times. The medical history is significant for the polycystic ovarian syndrome. The vital signs are as follows: temperature, 38.0°C (100.4°F); heart rate, 78/min; respiratory rate, 14/min; and blood pressure, 110/80 mm Hg. The family history is notable for paternal colon cancer. A colonoscopy is performed and is presented in the picture. A biopsy is taken from the affected area. What histologic findings are expected?
A 51-year-old man presents to his primary care physician's office for a 6-week history of fatigue and diarrhea. He says that the diarrhea is frequent, small volume, and contains gross blood. Review of systems is significant for subjective fever and an unintentional 5-pound weight loss. He denies recent travel outside of the United States. His past medical history is significant for IV drug abuse, HIV infection with non-compliance, and osteoarthritis. His family history is significant for Crohn disease in his mother. His temperature is 100.7°F (38.2°C), pulse is 90/min, blood pressure is 129/72 mmHg, and respirations are 16/min. His abdominal exam shows mild right and left lower quadrant tenderness with no rebound or guarding. Laboratory results are significant for a CD4 count of 42/mm^3. Colonoscopy with tissue biopsy will most likely reveal which of the following?
A 65-year-old man comes to the physician because of abdominal pain and bloody, mucoid diarrhea for 3 days. He has been taking over-the-counter supplements for constipation over the past 6 months. He was diagnosed with type 2 diabetes mellitus 15 years ago. He has smoked one pack of cigarettes daily for 35 years. His current medications include metformin. His temperature is 38.4°C (101.1°F), pulse is 92/min, and blood pressure is 134/82 mm Hg. Examination of the abdomen shows no masses. Palpation of the left lower abdomen elicits tenderness. A CT scan of the abdomen is shown. Which of the following is the most likely underlying cause of the patient's condition?

A 24-year-old woman comes to the physician because of progressively worsening episodes of severe, crampy abdominal pain and nonbloody diarrhea for the past 3 years. Examination of the abdomen shows mild distension and generalized tenderness. There is a fistula draining stool in the perianal region. Immunohistochemistry shows dysfunction of the nucleotide oligomerization binding domain 2 (NOD2) protein. This dysfunction most likely causes overactivity of which of the following immunological proteins in this patient?
A 52-year-old woman presents with mild epigastric pain and persistent heartburn for the past 2 months. An endoscopy is performed and reveals inflammation of the stomach mucosa without evidence of ulceration. A biopsy is performed and reveals intestinal metaplasia with destruction of a large number of parietal cells. She is diagnosed with chronic atrophic gastritis. Which of the following is characteristic of this patient’s diagnosis?
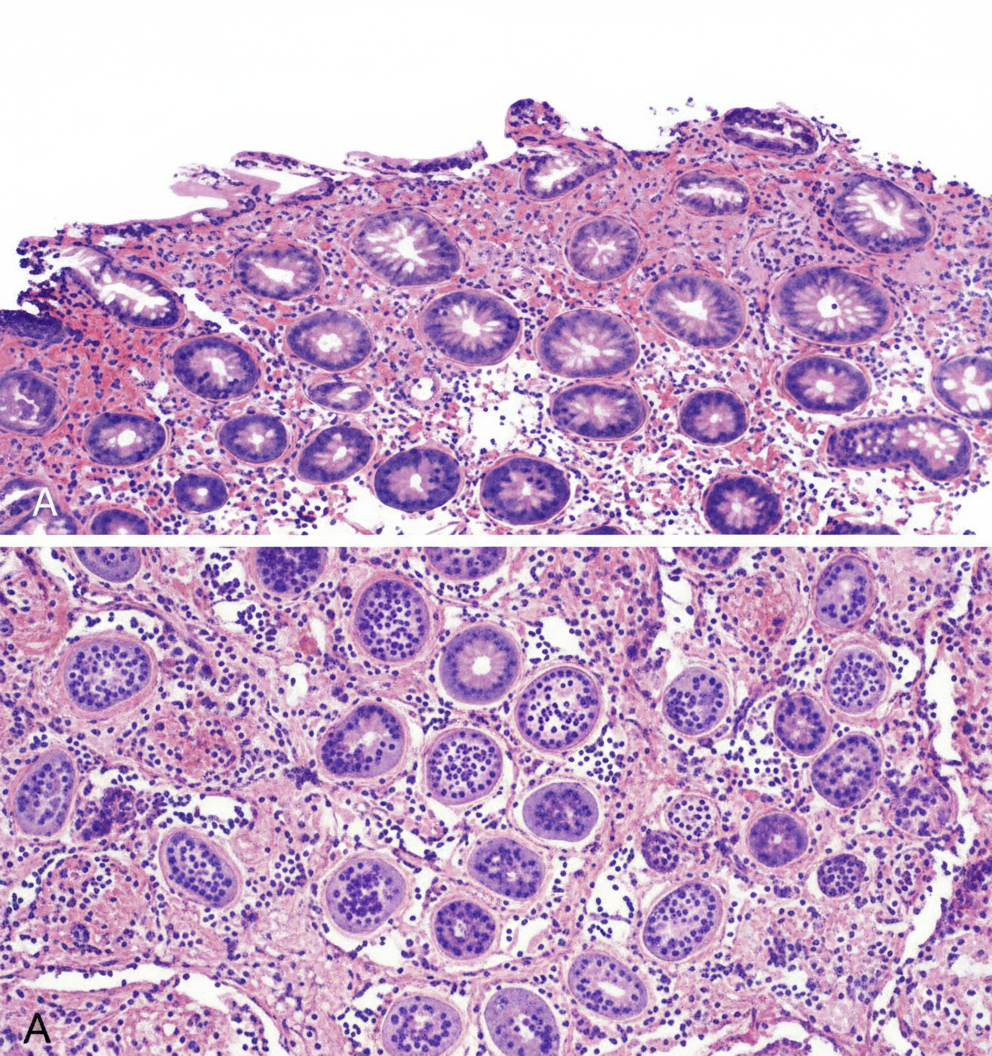
A 49-year-old woman presents to the primary care physician with complaints of recurrent episodes of right upper abdominal pain for the past 2 years. She is currently symptom-free. She mentions that the pain often occurs after a heavy fatty meal and radiates to her right shoulder. On examination, the patient has no tenderness in the abdomen and all other systemic examination is normal. Blood work shows: Leukocyte count 8,000/mm³ Total bilirubin 1.2 mg/dL Prothrombin time 12 s Aspartate transaminase 58 IU/L Alanine transaminase 61 IU/L Serum albumin 4.1 g/dL Stool occult blood negative Ultrasonography of the abdomen shows a thickened gallbladder wall with few gallstones. A hydroxy iminodiacetic acid (HIDA) scan was done which demonstrated non-filling of the gallbladder and a minimal amount of tracer in the common bile duct. Which of the following best describes a histopathological feature in the gallbladder described in this case?
A 67-year-old man with hypertension comes to the emergency department because of progressively worsening abdominal pain that started 1 week ago. The pain is localized to the right upper quadrant. He has also noticed yellowing of his eyes and skin during this time period. Physical examination shows jaundice, a distended abdomen, and tender hepatomegaly. There is no jugular venous distention. Laboratory studies show a hemoglobin concentration of 19.2 g/dL, aspartate aminotransferase of 420 U/L, alanine aminotransferase of 318 U/L, and total bilirubin of 2.2 mg/dL. Which of the following is the most likely cause of this patient's symptoms?
A 62-year-old woman with a history of hypertension, hyperlipidemia, and rheumatoid arthritis presents for evaluation of elevated serum liver chemistries. She has had three months of intense, unremitting itching. Current medications include chlorthalidone, atorvastatin, and ibuprofen. Physical exam is unremarkable. Laboratory studies show aspartate aminotransferase (AST) 42 units/L, alanine aminotransferase (ALT) 39 units/L, alkaline phosphatase 790 units/L, total bilirubin 0.8 mg/dL, and antimitochondrial antibody titer 1:80. What do you expect to see on liver biopsy?
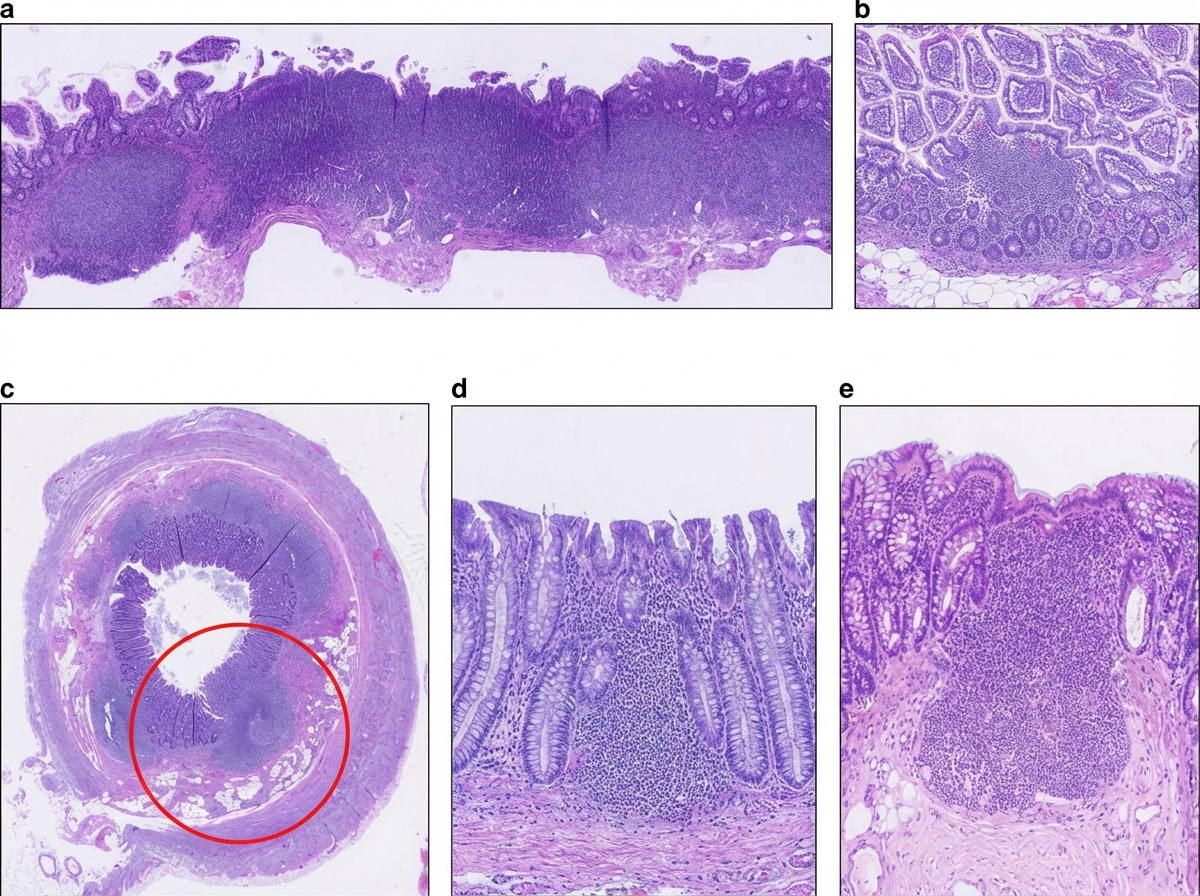
A 36-year-old man undergoes ileocecal resection after a gunshot injury. The resected ileocecal segment is sent for histological evaluation. One of the slides derived from the specimen is shown in the image. Which of the following statements regarding the structure marked within the red circle is correct?
Practice by Chapter
Esophageal pathology
Practice Questions
Gastritis and peptic ulcer disease
Practice Questions
Gastric tumors
Practice Questions
Malabsorption syndromes
Practice Questions
Inflammatory bowel diseases
Practice Questions
Intestinal infections
Practice Questions
Diverticular disease
Practice Questions
Vascular disorders of bowel
Practice Questions
Colon polyps and neoplasms
Practice Questions
Appendicitis
Practice Questions
Peritonitis
Practice Questions
Hernia complications
Practice Questions
Gastrointestinal stromal tumors
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app