
Malabsorption syndromes — MCQs

A 35-year-old Caucasian female presents with anemia, malaise, bloating, and diarrhea. Past genetic testing revealed that this patient carries the HLA-DQ2 allele. The physician suspects that the patient's presentation is dietary in cause. Which of the following findings would definitively confirm this diagnosis?
A 23-year-old man presents to the office complaining of weight loss and fatigue for the past 2 months. He states that he has been experiencing foul-smelling, light-colored stools but thinks it is because he hasn’t been eating well, recently. He has a past medical history significant for cystic fibrosis, which is well-controlled medically. He denies any shortness of breath, chest or abdominal pain, nausea, vomiting, or melena. On physical examination, his skin is pale and dry. Which of the following would be the most likely etiology of a malabsorption syndrome giving rise to this patient’s current condition?
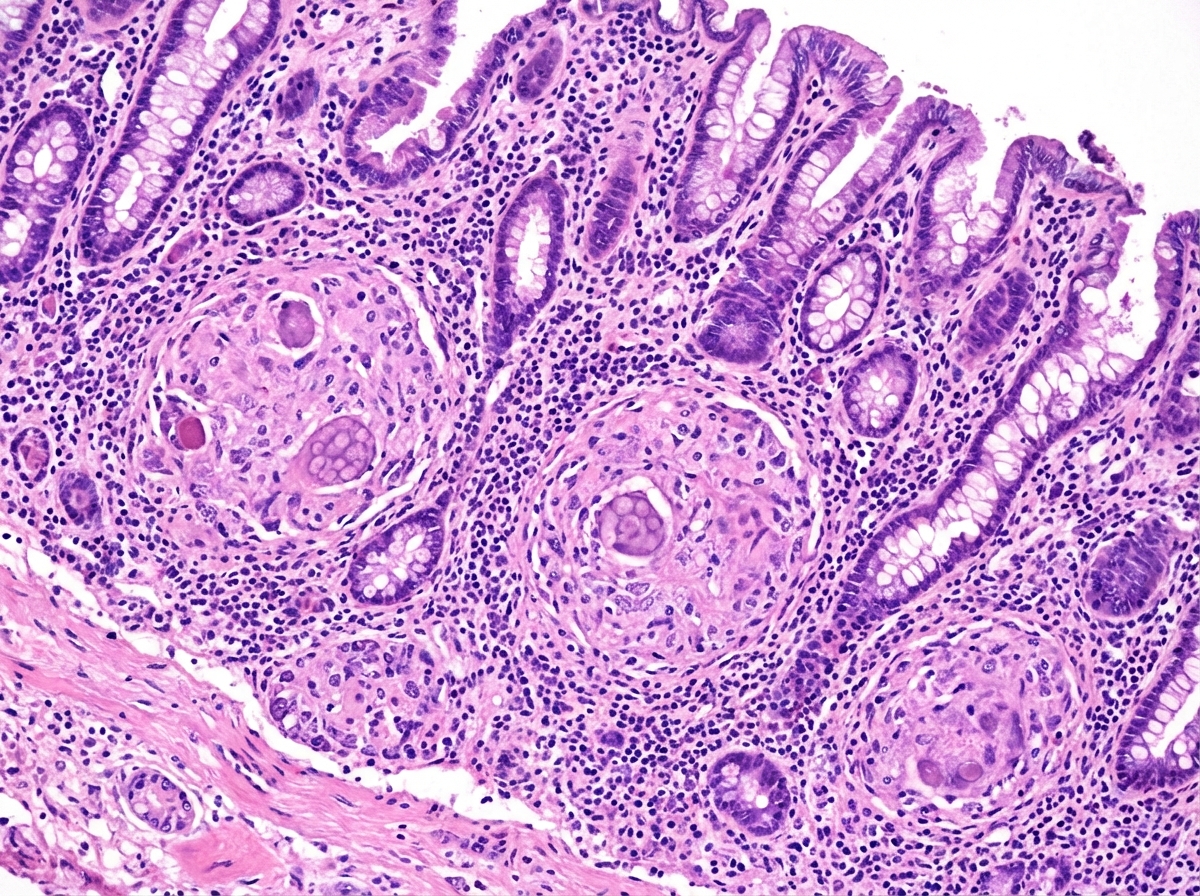
A 63-year-old man comes to the physician with a 4-week history of fatigue, crampy abdominal pain, watery diarrhea, and pain in his mouth and gums. He returned from a 2-week trip to the Dominican Republic 2 months ago. He has smoked one pack of cigarettes daily for 45 years. Examination shows three 1.5-cm, painful ulcers in the mouth. Abdominal examination shows mild tenderness to palpation in the right lower quadrant without guarding or rebound. His hemoglobin concentration is 11.2 g/dL, mean corpuscular volume is 75 fL, and leukocyte count is 11,900/mm³. Colonoscopy shows a cobblestone mucosa. A photomicrograph of a biopsy specimen is shown. Which of the following is the most likely diagnosis?
A 15-year-old girl is brought to the physician because of an 8-month history of fatigue, intermittent postprandial abdominal bloating and discomfort, foul-smelling, watery diarrhea, and a 7-kg (15-lb) weight loss. She developed a pruritic rash on her knees 3 days ago. Physical examination shows several tense, excoriated vesicles on the knees bilaterally. The abdomen is soft and nontender. Her hemoglobin concentration is 8.2 g/dL and mean corpuscular volume is 76 μm3. Further evaluation of this patient is most likely to show which of the following findings?
A previously healthy 20-year-old woman comes to the physician because of recurrent abdominal cramps, bloating, and diarrhea for 4 months. She describes her stools as greasy, foul-smelling, and difficult to flush. During this time she has had a 6-kg (13.2-lb) weight loss. She has no personal or family history of serious illness. Physical examination shows pallor and cheilitis. Laboratory studies show a hemoglobin concentration of 11 g/dL. Serum concentrations of electrolytes, urea nitrogen, and creatinine are within the reference range. Test of the stool for occult blood is negative and stool microscopy reveals no pathogens and no leukocytes. Analysis of a 24-hour stool sample shows 12 g of fat. The patient is asked to consume 25 g of d-xylose. Five hours later, its concentration is measured in urine at 2 g (N = > 4 g/5 h). The test is repeated after a two-week course of rifaximin, but the urinary concentration of d-xylose remains the same. Which of the following is the most likely diagnosis?
An 82-year-old woman presents with 2 months of foul-smelling, greasy diarrhea. She says that she also has felt very tired recently and has had some associated bloating and flatus. She denies any recent abdominal pain, nausea, melena, hematochezia, or vomiting. She also denies any history of recent travel and states that her home has city water. Which of the following tests would be most appropriate to initially work up the most likely diagnosis in this patient?
A 32-year-old woman presents with multiple pruritic papules and vesicles on her elbows and knees. She reports a history of gluten sensitivity. Skin biopsy shows granular IgA deposits in dermal papillae. Which of the following is most likely to be elevated in this patient's serum?
A 28-year-old male presents to his primary care physician with complaints of intermittent abdominal pain and alternating bouts of constipation and diarrhea. His medical chart is not significant for any past medical problems or prior surgeries. He is not prescribed any current medications. Which of the following questions would be the most useful next question in eliciting further history from this patient?
A 52-year-old man presents with 2 months of diarrhea, abdominal pain, and fatigue. He reports a weight loss of 4 kg (8 lb). He also says his joints have been hurting recently, as well. Past medical history is unremarkable. Review of systems is significant for problems with concentration and memory. Physical examination is unremarkable. A GI endoscopy is performed with a biopsy of the small bowel. Which of the following histologic finding would most likely be seen in this patient?
A 25-year-old male presents to his primary care physician for fatigue, abdominal pain, diarrhea, and weight loss. He states that this issue has occurred throughout his life but seems to “flare up” on occasion. He states that his GI pain is relieved with defecation, and his stools are frequent, large, and particularly foul-smelling. The patient has a past medical history of an ACL tear, as well as a car accident that resulted in the patient needing a transfusion and epinephrine to treat transfusion anaphylaxis. His current medications include vitamin D and ibuprofen. He recently returned from a camping trip in the eastern United States. He states that on the trip they cooked packed meats over an open fire and obtained water from local streams. His temperature is 99.5°F (37.5°C), blood pressure is 120/77 mmHg, pulse is 70/min, respirations are 11/min, and oxygen saturation is 98% on room air. Physical exam reveals poor motor control and an ataxic gait on neurologic exam. Cardiac and pulmonary exams are within normal limits. Laboratory studies are ordered and return as below: Hemoglobin: 9.0 g/dL Hematocrit: 25% Haptoglobin: 12 mg/dL Leukocyte count: 7,500 cells/mm^3 with normal differential Platelet count: 255,000/mm^3 Serum: Na+: 140 mEq/L Cl-: 102 mEq/L K+: 5.0 mEq/L HCO3-: 24 mEq/L BUN: 24 mg/dL Glucose: 82 mg/dL Creatinine: 1.0 mg/dL Ca2+: 9.0 mg/dL LDH: 457 U/L AST: 11 U/L ALT: 11 U/L Radiography is ordered which reveals a stress fracture in the patient’s left tibia. Which of the following is the best confirmatory test for this patient’s condition?
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app