
Esophageal pathology — MCQs

A 23-year-old college senior visits the university health clinic after vomiting large amounts of blood. He has been vomiting for the past 36 hours after celebrating his team’s win at the national hockey championship with his varsity friends while consuming copious amounts of alcohol. His personal medical history is unremarkable. His blood pressure is 129/89 mm Hg while supine and 100/70 mm Hg while standing. His pulse is 98/min, strong and regular, with an oxygen saturation of 98%. His body temperature is 36.5°C (97.7°F), while the rest of the physical exam is normal. Which of the following is associated with this patient’s condition?
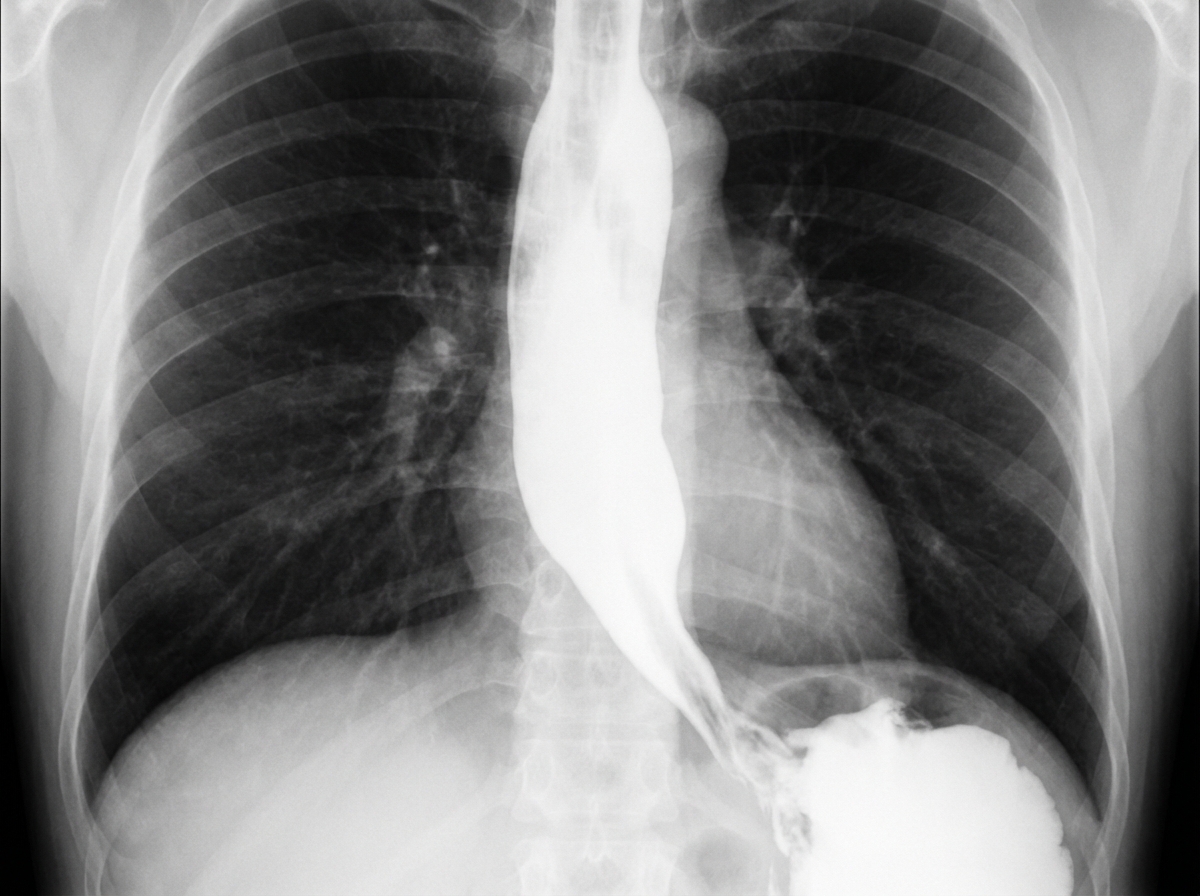
A 62-year-old man is referred to a gastroenterologist because of difficulty swallowing for the past 5 months. He has difficulty swallowing both solid and liquid foods, but there is no associated pain. He denies any shortness of breath or swelling in his legs. He immigrated from South America 10 years ago. He is a non-smoker and does not drink alcohol. His physical examination is unremarkable. A barium swallow study was ordered and the result is given below. Esophageal manometry confirms the diagnosis. What is the most likely underlying cause of this patient’s condition?
A 25-year-old man presents to the emergency department after numerous episodes of vomiting. The patient states that he thinks he ‘ate something weird’ and has been vomiting for the past 48 hours. He says that he came to the hospital because the last few times he "threw up blood". He is hypotensive with a blood pressure of 90/55 mm Hg and a pulse of 120/min. After opening an intravenous line, a physical examination is performed which is normal except for mild epigastric tenderness. An immediate endoscopy is performed and a tear involving the mucosa and submucosa of the gastroesophageal junction is visualized. Which of the following is the most likely diagnosis?
A 45-year-old man comes to the physician for the evaluation of painful swallowing and retrosternal pain over the past 2 days. He was recently diagnosed with HIV infection, for which he now takes tenofovir, emtricitabine, and raltegravir. There is no family history of serious illness. He has smoked one pack of cigarettes daily for the past 20 years. He drinks 2–3 beers per day. He does not use illicit drugs. Vital signs are within normal limits. Physical examination of the oral cavity shows no abnormalities. The patient's CD4+ T-lymphocyte count is 80/mm3 (normal ≥ 500). Empiric treatment is started. Two weeks later, he reports no improvement in his symptoms. Esophagogastroduodenoscopy is performed and shows multiple well-circumscribed, round, superficial ulcers in the upper esophagus. Which of the following is the most likely underlying cause of this patient's symptoms?
An 85-year-old man who recently immigrated to the US from Spain presents to your office complaining of hoarseness and dysphagia for the past 2 months. He says his symptoms have been getting progressively worse, and he expresses concerns about the difficulty swallowing as he cannot eat well and has even lost 9 kg (20 lb) since his last visit 3 months ago. He denies any shortness of breath, coughing of blood, and chest pain. His bowel and bladder habit are normal. Past medical history is unremarkable. He has a 60-pack-year history of smoking tobacco and drinks alcohol occasionally. Which of the following is the most likely cause of his symptoms?
A 65-year-old African-American man presents to your office with dysphagia. He reports that he has found it progressively more difficult to swallow food over the past year. At the time of presentation, he is able to eat only soup. Social history is significant for asbestos exposure, multiple daily drinks of hard alcohol, and a 70 pack-year smoking history. What would you most expect to see on an esophageal biopsy of this patient?
A 56-year-old man comes to the physician because of intermittent retrosternal chest pain. Physical examination shows no abnormalities. Endoscopy shows salmon pink mucosa extending 5 cm proximal to the gastroesophageal junction. Biopsy specimens from the distal esophagus show nonciliated columnar epithelium with numerous goblet cells. Which of the following is the most likely cause of this patient's condition?
A 28-year-old male presents to his primary care physician with complaints of intermittent abdominal pain and alternating bouts of constipation and diarrhea. His medical chart is not significant for any past medical problems or prior surgeries. He is not prescribed any current medications. Which of the following questions would be the most useful next question in eliciting further history from this patient?
A 47-year-old woman presents for a routine wellness checkup. She complains of general fatigue and lethargy for the past 6 months. She does not have a significant past medical history and is currently not taking any medications. The patient reports that she drinks “socially” approx. 6 nights a week. She says she also enjoys a “nightcap,” which is 1–2 glasses of wine before bed every night. She denies any history of drug use or smoking. The patient is afebrile, and her vital signs are within normal limits. A physical examination reveals pallor of the mucous membranes. Her laboratory findings are significant for a mean corpuscular volume of 72 fL, leukocyte count of 5,300/mL, hemoglobin of 11.0 g/dL, and platelet count of 420,000/mL. Which of the following is the most likely cause of this patient’s thrombocytosis?
A 61-year-old man with a history of stage IIIa lung adenocarcinoma that has been treated with wedge resection and chemotherapy presents to the primary care clinic. He is largely asymptomatic, but he demonstrates a persistent microcytic anemia despite iron supplementation. Colonoscopy performed 3 years earlier was unremarkable. His past medical history is significant for diabetes mellitus type II, hypertension, acute lymphoblastic leukemia as a child, and hypercholesterolemia. He currently smokes 1 pack of cigarettes per day, drinks a glass of pinot grigio per day, and currently denies any illicit drug use. His vital signs include: temperature, 36.7°C (98.0°F); blood pressure, 126/74 mm Hg; heart rate, 87/min; and respiratory rate, 17/min. On physical examination, his pulses are bounding, complexion is pale, but breath sounds remain clear. Oxygen saturation was initially 91% on room air, with a new oxygen requirement of 2 L by nasal cannula. Which of the following lab values would suggest anemia of chronic disease as the underlying etiology?
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app