
Diverticular disease — MCQs

A 72-year-old female presents to the emergency department complaining of severe abdominal pain and several days of bloody diarrhea. Her symptoms began with intermittent bloody diarrhea five days ago and have worsened steadily. For the last 24 hours, she has complained of fevers, chills, and abdominal pain. She has a history of ulcerative colitis, idiopathic hypertension, and hypothyroidism. Her medications include hydrochlorothiazide, levothyroxine, and sulfasalazine. In the ED, her temperature is 39.1°C (102.4°F), pulse is 120/min, blood pressure is 90/60 mmHg, and respirations are 20/min. On exam, the patient is alert and oriented to person and place, but does not know the day. Her mucus membranes are dry. Heart and lung exam are not revealing. Her abdomen is distended with marked rebound tenderness. Bowel sounds are hyperactive. Serum: Na+: 142 mEq/L Cl-: 107 mEq/L K+: 3.3 mEq/L HCO3-: 20 mEq/L BUN: 15 mg/dL Glucose: 92 mg/dL Creatinine: 1.2 mg/dL Calcium: 10.1 mg/dL Hemoglobin: 11.2 g/dL Hematocrit: 30% Leukocyte count: 14,600/mm^3 with normal differential Platelet count: 405,000/mm^3 What is the next best step in management?
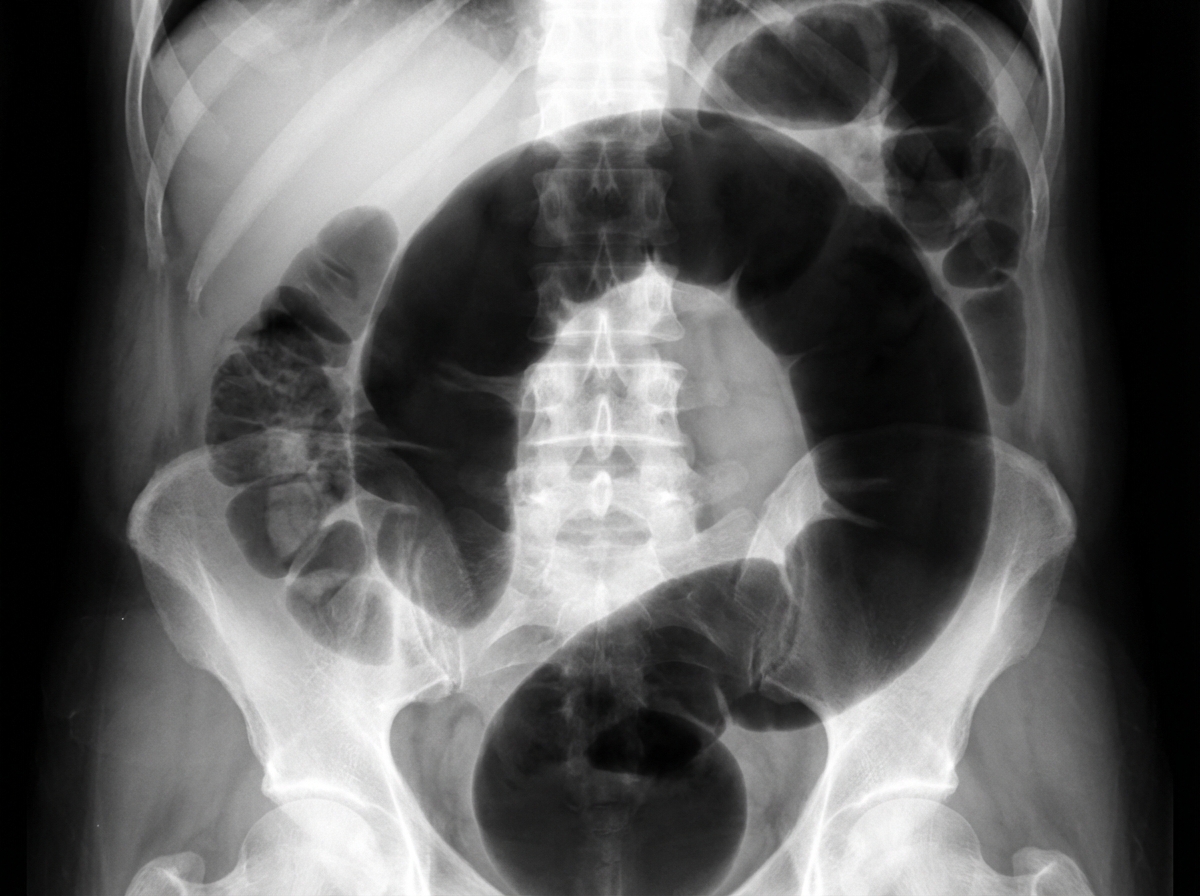
A 46-year-old woman comes to the emergency department because of intermittent abdominal pain and vomiting for 2 days. The abdominal pain is colicky and diffuse. The patient's last bowel movement was 3 days ago. She has had multiple episodes of upper abdominal pain that radiates to her scapulae and vomiting over the past 3 months; her symptoms subsided after taking ibuprofen. She has coronary artery disease, type 2 diabetes mellitus, gastroesophageal reflux disease, and osteoarthritis of both knees. Current medications include aspirin, atorvastatin, rabeprazole, insulin, and ibuprofen. She appears uncomfortable. Her temperature is 39°C (102.2°F), pulse is 111/min, and blood pressure is 108/68 mm Hg. Examination shows dry mucous membranes. The abdomen is distended and tympanitic with diffuse tenderness; bowel sounds are high-pitched. Rectal examination shows a collapsed rectum. Her hemoglobin concentration is 13.8 g/dL, leukocyte count is 14,400/mm3, and platelet count is 312,000/mm3. An x-ray of the abdomen is shown. Which of the following is the most likely cause of this patient's findings?

A 68-year-old woman is brought to the emergency department with intense abdominal pain for the past 2 hours. She has had 1 episode of bloody diarrhea recently. She has an 18-year history of diabetes mellitus. She was diagnosed with hypertension and ischemic heart disease 6 years ago. She is fully alert and oriented. Her temperature is 37.5°C (99.5°F), blood pressure is 145/90 mm Hg, pulse is 78/min, and respirations are 14/min. Abdominal examination shows mild generalized abdominal tenderness without guarding or rebound tenderness. An abdominal plain X-ray shows no abnormalities. Abdominal CT reveals colonic wall thickening and pericolonic fat stranding in the splenic curvature. Bowel rest, intravenous hydration, and IV antibiotics are initiated. Which of the following is the most important diagnostic evaluation at this time?
A 75-year-old man presents to the emergency department for abdominal pain. The patient states the pain started this morning and has been worsening steadily. He decided to come to the emergency department when he began vomiting. The patient has a past medical history of obesity, diabetes, alcohol abuse, and hypertension. His current medications include captopril, insulin, metformin, sodium docusate, and ibuprofen. His temperature is 104.0°F (40°C), blood pressure is 160/97 mmHg, pulse is 90/min, respirations are 15/min, and oxygen saturation is 98% on room air. Abdominal exam reveals left lower quadrant tenderness. Cardiac exam reveals a crescendo systolic murmur heard best by the right upper sternal border. Lab values are ordered and return as below. Hemoglobin: 15 g/dL Hematocrit: 42% Leukocyte count: 19,500 cells/mm^3 with normal differential Platelet count: 226,000/mm^3 Serum: Na+: 139 mEq/L Cl-: 101 mEq/L K+: 4.4 mEq/L HCO3-: 24 mEq/L BUN: 22 mg/dL Glucose: 144 mg/dL Creatinine: 1.2 mg/dL Ca2+: 9.8 mg/dL Which of the following is the most accurate test for this patient's condition?
An institutionalized 65-year-old man is brought to the emergency department because of abdominal pain and distension for 12 hours. The pain was acute in onset and is a cramping-type pain associated with nausea, vomiting, and constipation. He has a history of chronic constipation and has used laxatives for years. There is no history of inflammatory bowel disease in his family. He has not been hospitalized recently. There is no recent history of weight loss or change in bowel habits. On physical examination, the patient appears ill. The abdomen is distended with tenderness mainly in the left lower quadrant and is tympanic on percussion. The blood pressure is 110/79 mm Hg, heart rate is 100/min, the respiratory rate is 20/min, and the temperature is 37.2°C (99.0°F). The CBC shows an elevated white blood cell count. The plain abdominal X-ray is shown in the accompanying image. What is the most likely cause of his condition?
A 70-year-old man with a history of chronic constipation presents to the emergency department with a two-day history of left lower quadrant abdominal pain. He is found to have a temperature of 100.8F, BP 140/90, HR 85, and RR 16. On physical examination, he is tender to light palpation in the left lower quadrant and exhibits voluntary guarding. Rectal examination reveals heme-positive stool. Laboratory values are unremarkable except for a WBC count of 12,500 with a left shift. Which of the following tests would be most useful in the diagnosis of this patient's disease?
A 25-year-old male presents to his primary care physician for fatigue, abdominal pain, diarrhea, and weight loss. He states that this issue has occurred throughout his life but seems to “flare up” on occasion. He states that his GI pain is relieved with defecation, and his stools are frequent, large, and particularly foul-smelling. The patient has a past medical history of an ACL tear, as well as a car accident that resulted in the patient needing a transfusion and epinephrine to treat transfusion anaphylaxis. His current medications include vitamin D and ibuprofen. He recently returned from a camping trip in the eastern United States. He states that on the trip they cooked packed meats over an open fire and obtained water from local streams. His temperature is 99.5°F (37.5°C), blood pressure is 120/77 mmHg, pulse is 70/min, respirations are 11/min, and oxygen saturation is 98% on room air. Physical exam reveals poor motor control and an ataxic gait on neurologic exam. Cardiac and pulmonary exams are within normal limits. Laboratory studies are ordered and return as below: Hemoglobin: 9.0 g/dL Hematocrit: 25% Haptoglobin: 12 mg/dL Leukocyte count: 7,500 cells/mm^3 with normal differential Platelet count: 255,000/mm^3 Serum: Na+: 140 mEq/L Cl-: 102 mEq/L K+: 5.0 mEq/L HCO3-: 24 mEq/L BUN: 24 mg/dL Glucose: 82 mg/dL Creatinine: 1.0 mg/dL Ca2+: 9.0 mg/dL LDH: 457 U/L AST: 11 U/L ALT: 11 U/L Radiography is ordered which reveals a stress fracture in the patient’s left tibia. Which of the following is the best confirmatory test for this patient’s condition?
A 41-year-old male who takes NSAIDs regularly for his chronic back pain develops severe abdominal pain worse with eating. Upper endoscopy is performed and the medical student asks the supervising physician how the histological differentiation between a gastric ulcer and erosion is made. Which of the following layers of the gastric mucosa MUST be breached for a lesion to be considered an ulcer?
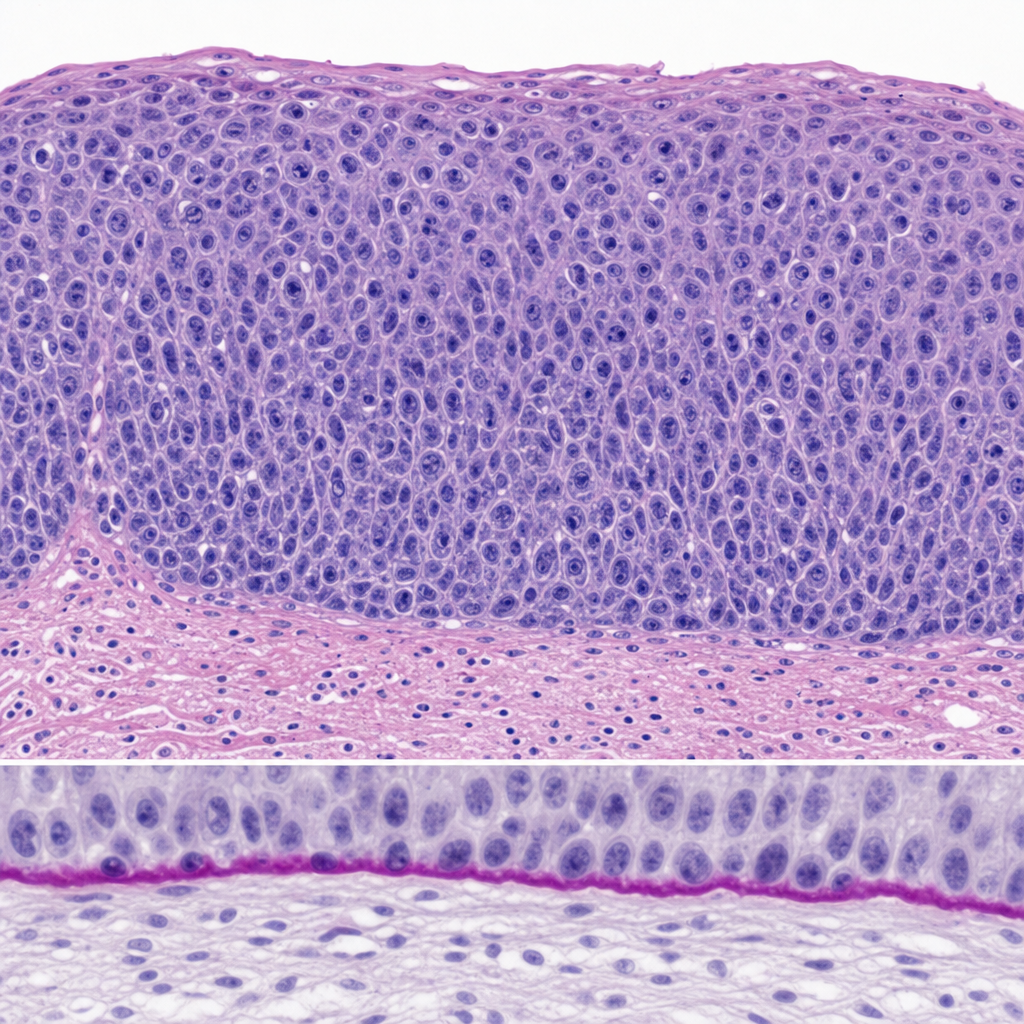
A 34-year-old woman undergoes excisional biopsy of a cervical lesion detected on colposcopy. The photomicrograph demonstrates full-thickness replacement of the squamous epithelium by atypical cells with high nuclear-to-cytoplasmic ratios, loss of polarity, and numerous mitotic figures extending to the surface. The basement membrane appears intact on PAS stain. Which of the following statements most accurately characterizes the biological behavior of this lesion?
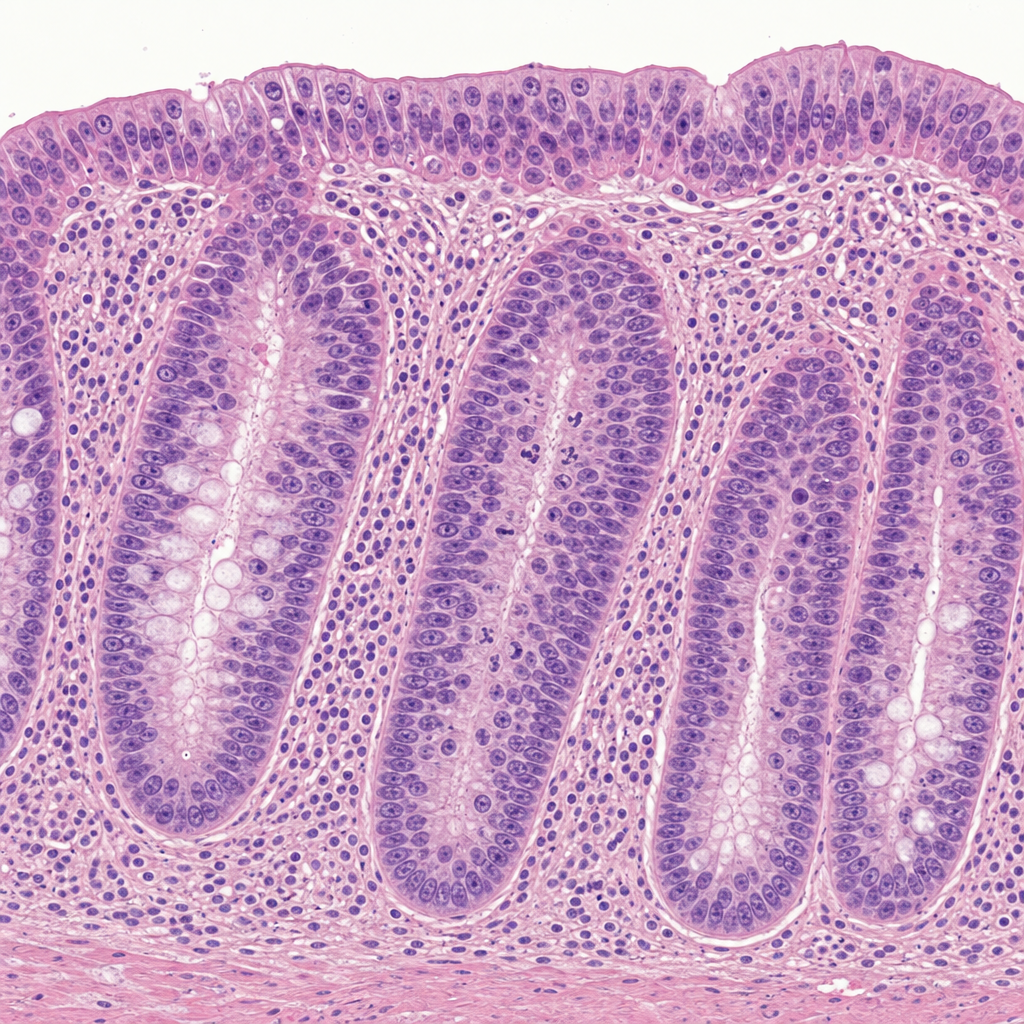
A 38-year-old woman with a history of ulcerative colitis for 12 years undergoes surveillance colonoscopy. A flat mucosal lesion is biopsied from the sigmoid colon. The photomicrograph shows colonic crypts with enlarged, hyperchromatic, stratified nuclei that extend to the luminal surface; nuclear polarity is partially lost; there is increased mitotic activity; and the basement membrane is intact with no extension of atypical cells into the lamina propria. Which of the following statements best characterizes the biological behavior of this lesion?
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app