
GI — MCQs

On this page
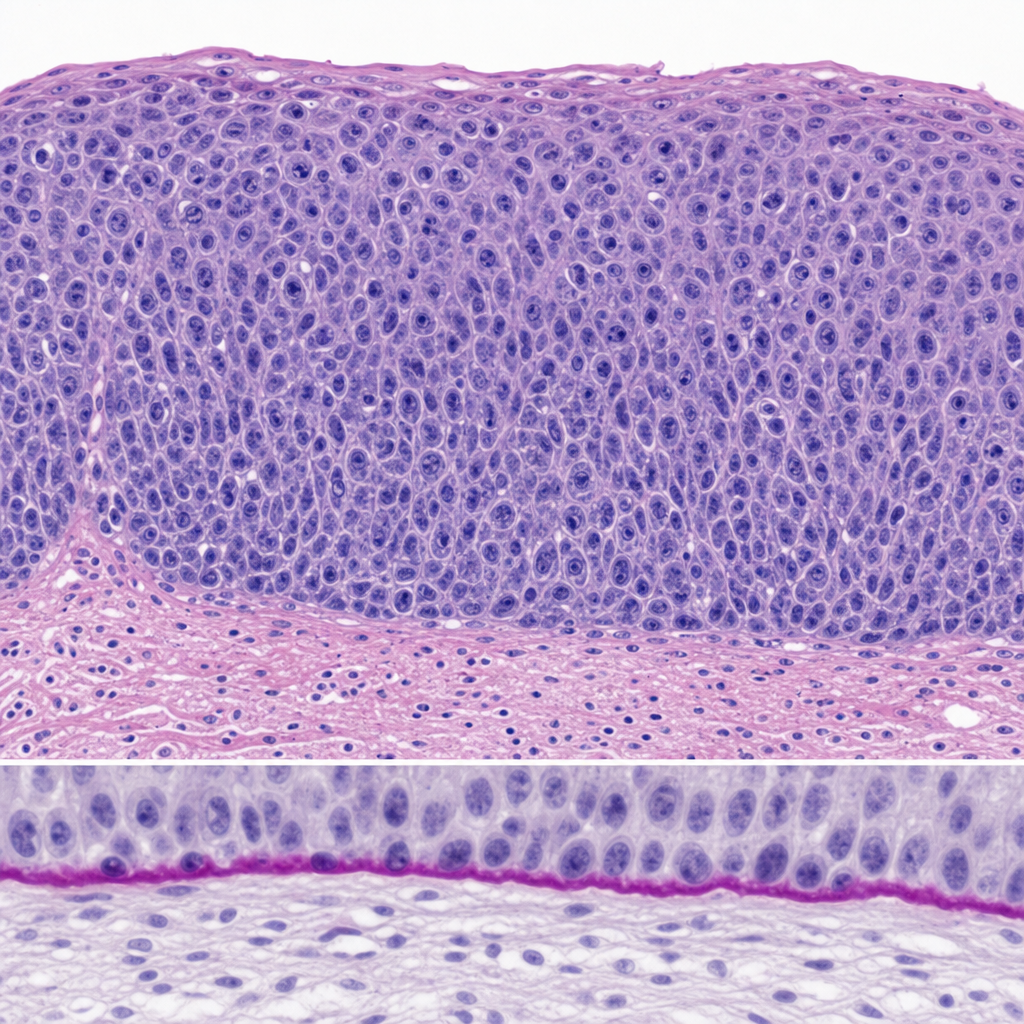
A 34-year-old woman undergoes excisional biopsy of a cervical lesion detected on colposcopy. The photomicrograph demonstrates full-thickness replacement of the squamous epithelium by atypical cells with high nuclear-to-cytoplasmic ratios, loss of polarity, and numerous mitotic figures extending to the surface. The basement membrane appears intact on PAS stain. Which of the following statements most accurately characterizes the biological behavior of this lesion?
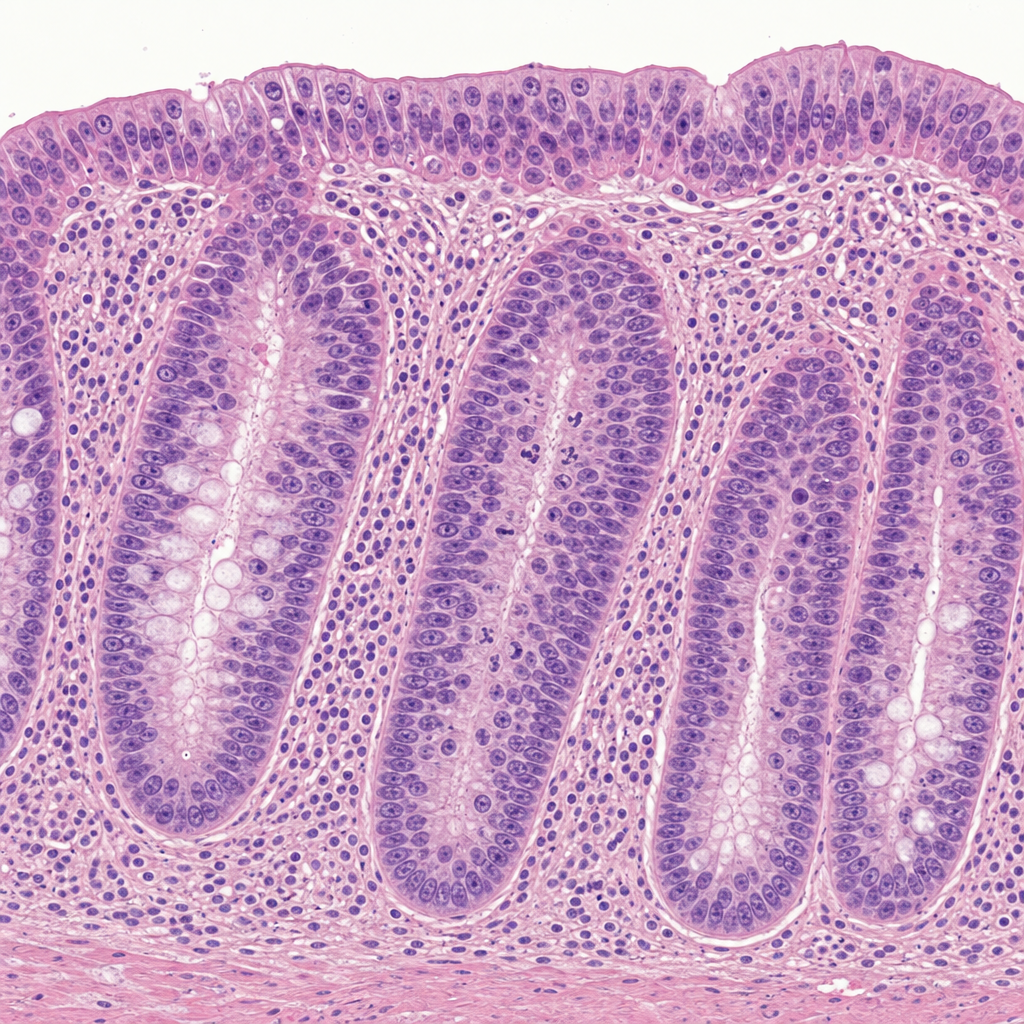
A 38-year-old woman with a history of ulcerative colitis for 12 years undergoes surveillance colonoscopy. A flat mucosal lesion is biopsied from the sigmoid colon. The photomicrograph shows colonic crypts with enlarged, hyperchromatic, stratified nuclei that extend to the luminal surface; nuclear polarity is partially lost; there is increased mitotic activity; and the basement membrane is intact with no extension of atypical cells into the lamina propria. Which of the following statements best characterizes the biological behavior of this lesion?
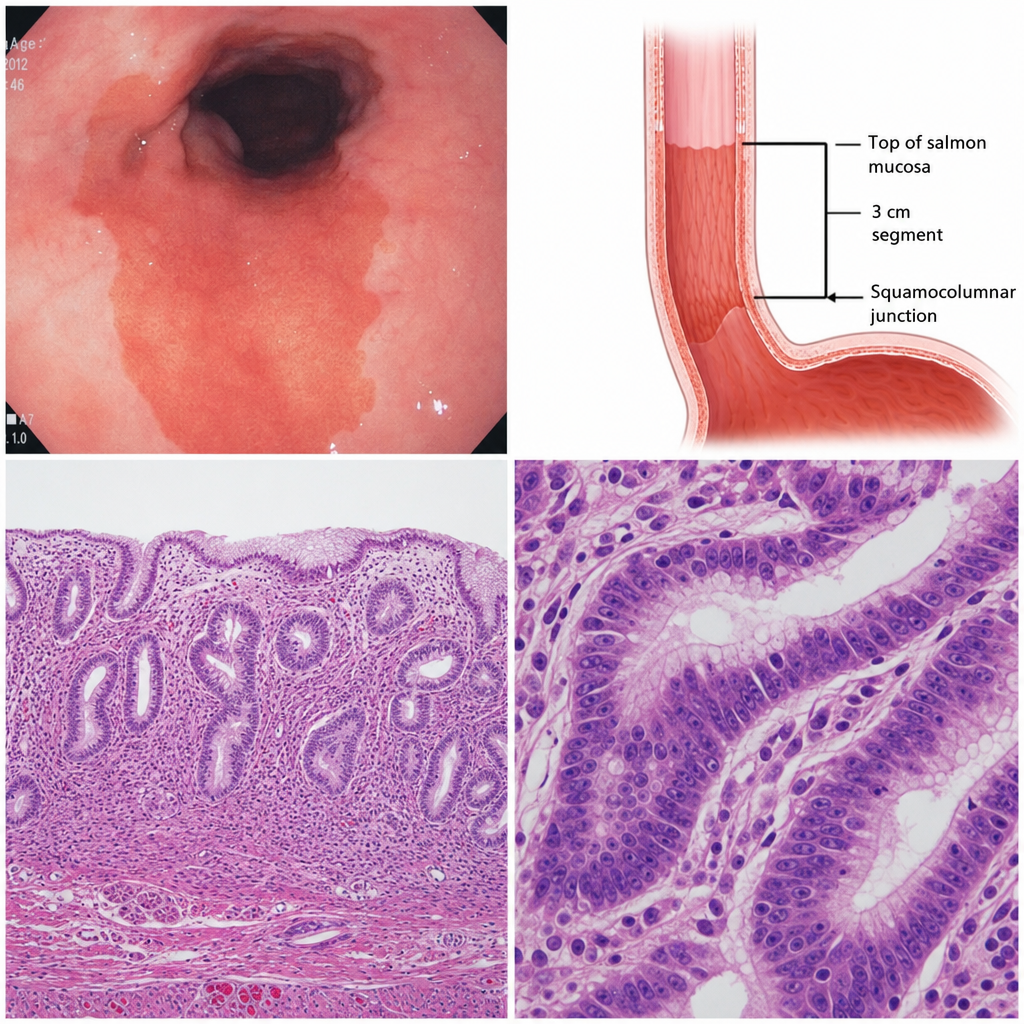
A 45-year-old woman with a history of chronic gastroesophageal reflux disease undergoes upper endoscopy. The gastroesophageal junction mucosa appears salmon-pink and velvety, extending 3 cm above the squamocolumnar junction. Biopsy is taken from this region. A subsequent biopsy taken one year later shows the same columnar epithelium with nuclear crowding, loss of polarity, and architectural complexity confined entirely above the basement membrane. Which of the following correctly describes the biological behavior of the change seen on the second biopsy?
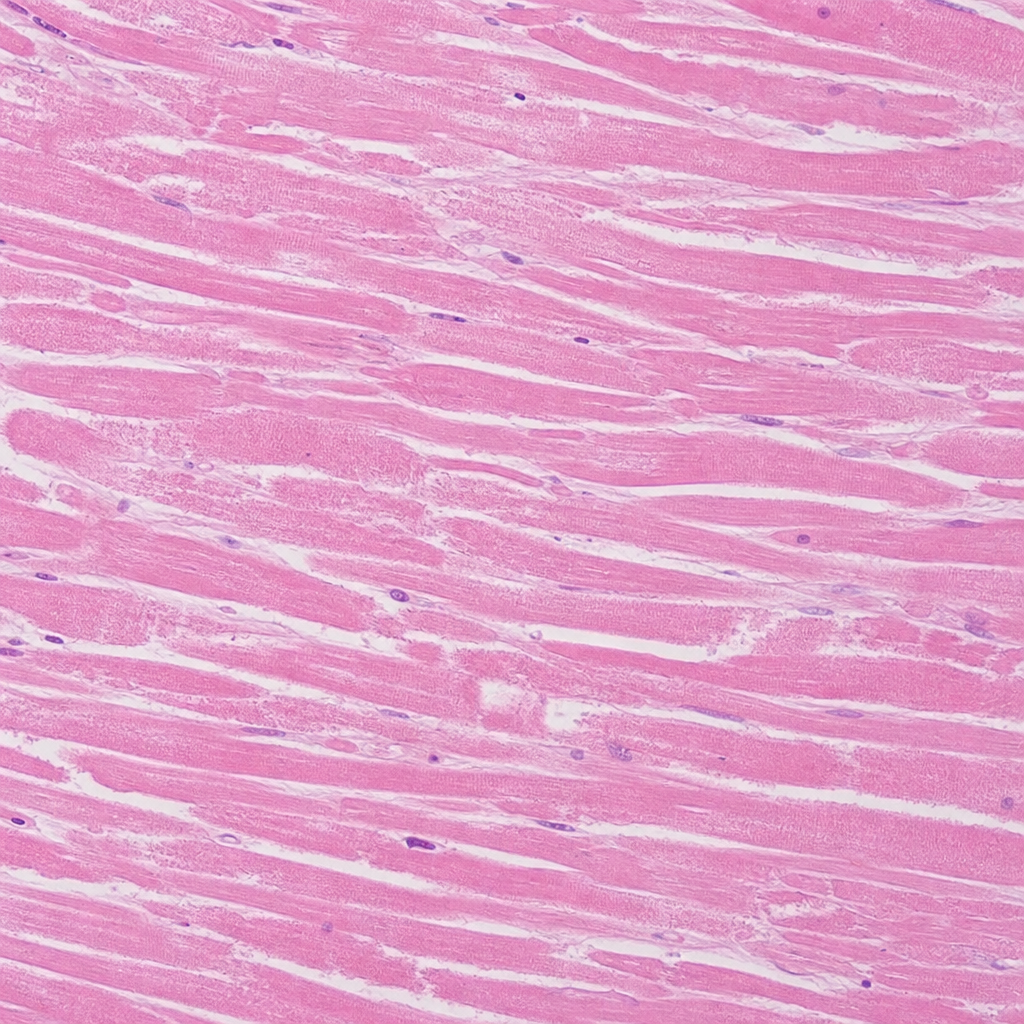
A 62-year-old man with a 40 pack-year smoking history dies suddenly. At autopsy, a large transmural infarct is identified in the left anterior descending artery territory. Histological sections from the center of the infarct are taken. The photomicrograph shows preserved cellular outlines with loss of nuclei and cytoplasmic eosinophilia, but no neutrophilic infiltrate is visible. No neutrophil margination is identified at the infarct periphery. Which of the following best estimates the age of this infarct, and which morphological feature most directly supports that estimate?
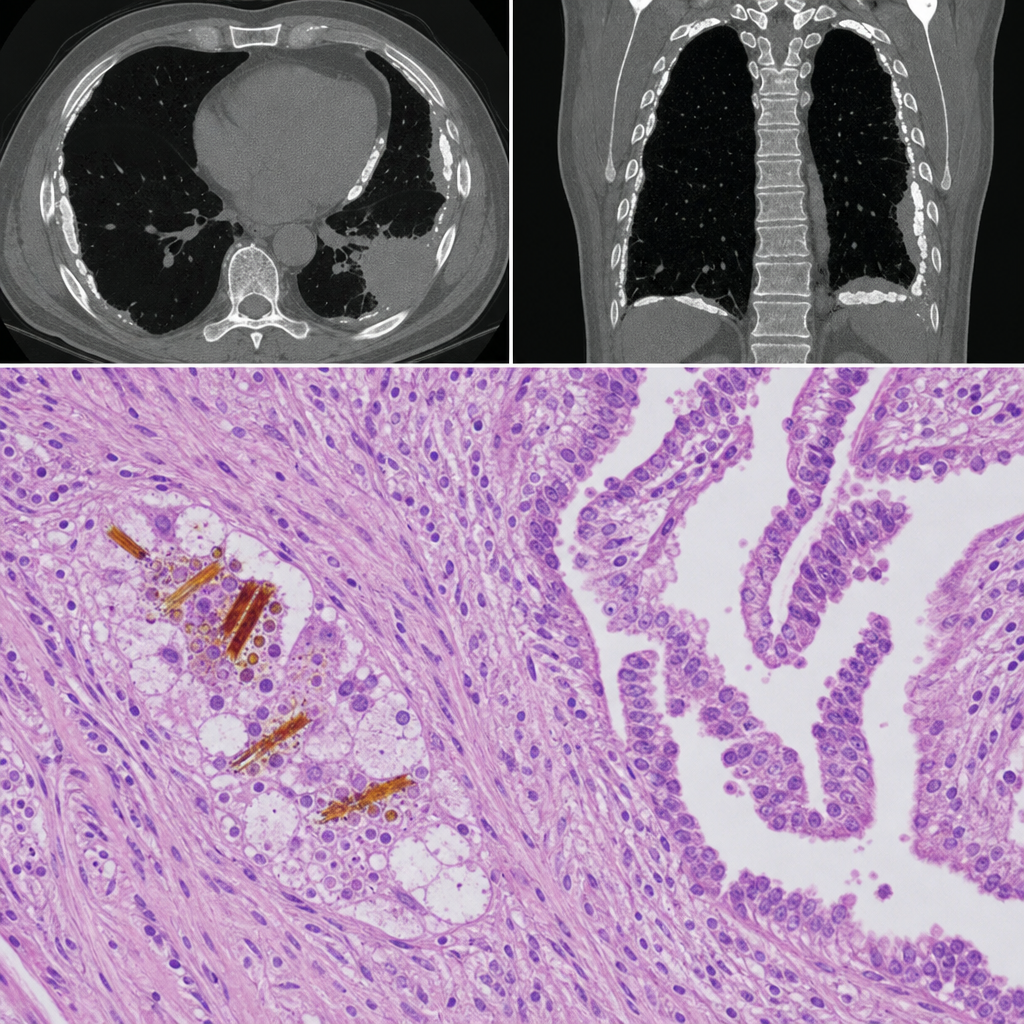
A 58-year-old man with a 40-pack-year smoking history presents with progressive dyspnea and a dry cough. Chest CT reveals bilateral pleural plaques and a pleural-based mass. A pleural biopsy is performed. The photomicrograph shows elongated, beaded, golden-brown structures within macrophages in the lung parenchyma adjacent to the mass, surrounded by a biphasic proliferation of epithelioid and spindle cells arranged in a tubulopapillary pattern. Which of the following best describes the golden-brown structures seen in this biopsy?
A 52-year-old man, with a history of alcoholism, presents with loss of appetite, abdominal pain, and fever for the past 24 hours. He says he consumed 12 beers and a bottle of vodka 2 days ago. He reports a 19-year history of alcoholism. His blood pressure is 100/70 mm Hg, pulse is 100/min, respirations are 20/min, and oxygen saturation is 99% on room air. Laboratory findings are significant for the following: Sodium 137 mEq/L Potassium 3.4 mEq/L Alanine aminotransferase (ALT) 230 U/L Aspartate aminotransferase (AST) 470 U/L Which of the following histopathologic findings would most likely be found on a liver biopsy of this patient?
A 25-year-old woman presents to her primary care physician complaining of several months of diarrhea. She has also had crampy abdominal pain. She has tried modifying her diet without improvement. She has many watery, non-bloody bowel movements per day. She also reports feeling fatigued. The patient has not recently traveled outside of the country. She has lost 10 pounds since her visit last year, and her BMI is now 20. On exam, she has skin tags and an anal fissure. Which of the following would most likely be seen on endoscopy and biopsy?
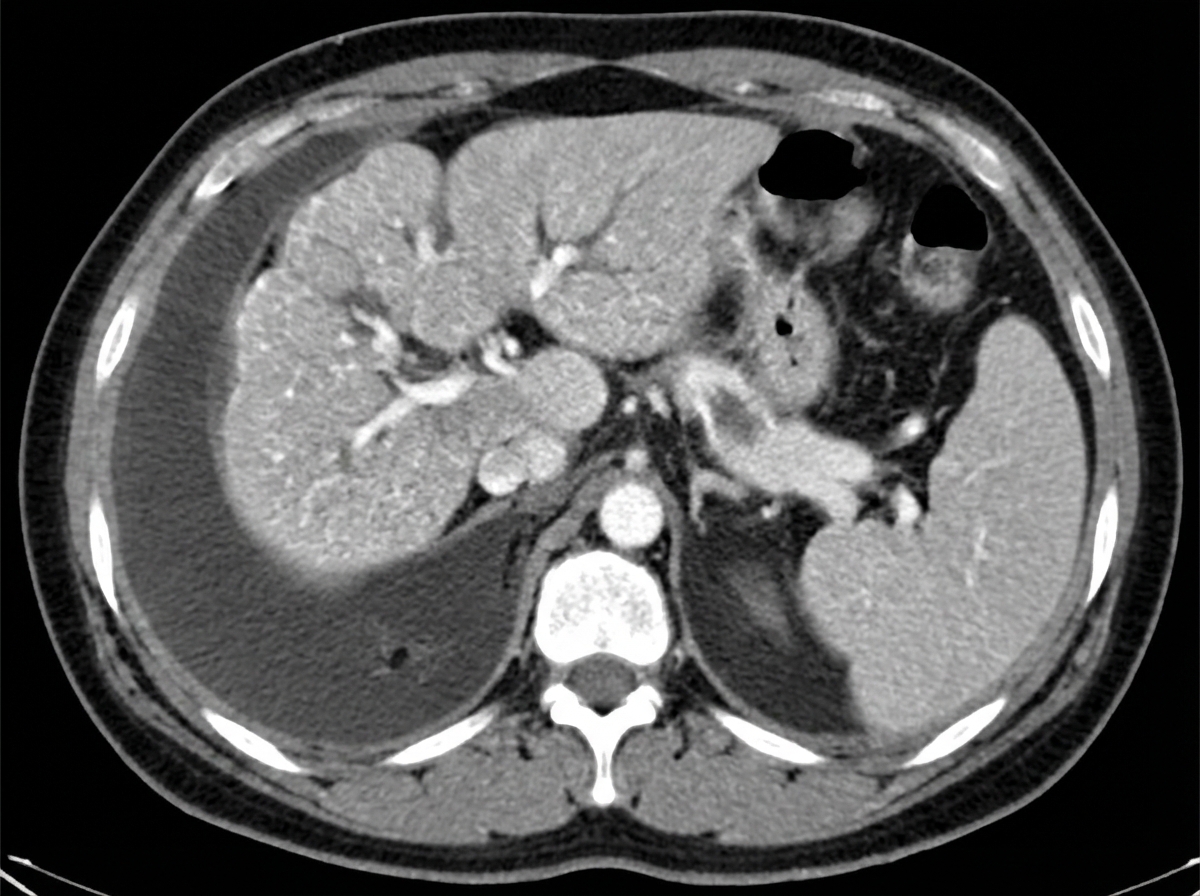
A 65-year-old man is brought to the emergency department because of a 1-day history of fever and disorientation. His wife reports that he had abdominal pain and diarrhea the previous day. He drinks 60 oz of alcohol weekly. His pulse is 110/min and blood pressure is 96/58 mm Hg. Examination shows jaundice, palmar erythema, spider nevi on his chest, dilated veins on the anterior abdominal wall, and 2+ edema of the lower extremities. The abdomen is soft and diffusely tender; there is shifting dullness to percussion. His albumin is 1.4 g/dL, bilirubin is 5 mg/dL, and prothrombin time is 31 seconds (INR = 3.3). Hepatitis serology is negative. A CT scan of the abdomen is shown. Which of the following processes is the most likely explanation for these findings?
An esophageal biopsy sample from a 47-year-old male with chronic heartburn reveals intestinal metaplasia. Which of the following abnormal cell types is likely present in this patient's esophagus?
A 21-year-old man comes to the physician because of a 6-month history of severe abdominal pain, bloating, and episodic diarrhea. He has also had a 5-kg (11-lb) weight loss during this time. Physical examination shows a mildly distended abdomen, hyperactive bowel sounds, and diffuse abdominal tenderness. A biopsy specimen of the colonic mucosa shows scattered areas of inflammation with fibrosis and noncaseating granulomas. Which of the following is most likely involved in the pathogenesis of this patient's condition?
Practice by Chapter
Esophageal pathology
Practice Questions
Gastritis and peptic ulcer disease
Practice Questions
Gastric tumors
Practice Questions
Malabsorption syndromes
Practice Questions
Inflammatory bowel diseases
Practice Questions
Intestinal infections
Practice Questions
Diverticular disease
Practice Questions
Vascular disorders of bowel
Practice Questions
Colon polyps and neoplasms
Practice Questions
Appendicitis
Practice Questions
Peritonitis
Practice Questions
Hernia complications
Practice Questions
Gastrointestinal stromal tumors
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app