
General Pathology — MCQs

On this page
A 35-year-old woman is involved in a car accident and presents with an open fracture of the left femur and severe bleeding from the left femoral artery. No past medical history or current medications. Her blood pressure is 90/60 mm Hg, pulse is 110/min, and respirations are 21/min. On physical examination, the patient is lethargic, confused, and poorly responds to commands. Peripheral pulses are 1+ in the left lower extremity below the level of the knee and 2+ elsewhere. When she arrives at the hospital, a stat hemoglobin level shows 6 g/dL. Which of the following is most correct about the patient’s condition?
A 35-year-old man is brought to the emergency room after suffering a catastrophic fall while skiing during a training session. He was found unconscious by the aeromedical emergency services team, who established an airway and cervical spine control measures. Upon arrival at the emergency department, ventilatory support is started followed by an evaluation of the patient by the neurosurgical team. His blood pressure is 210/125 mm Hg, the heart rate is 55/min, and the respiratory rate is 15/min with a Cheyne-Stokes breathing pattern. Neurological examination shows a Glasgow Coma Score of 4/15, with dilated, fixed pupils and a decerebrate posture. An MRI of the brain shows diffuse axonal injury to the brain with severe cerebral edema, multiple frontal and occipital lobe contusions and multiple flame-shaped hemorrhages in the brainstem. Despite the medical team efforts, the patient dies 24 hours later. What would be the most likely type of herniation found at this patient’s autopsy?
A newborn male is evaluated in the hospital nursery two hours after birth. The patient was born at 39 weeks of gestation to a 30-year-old primigravid via vaginal delivery. The patient’s mother received routine prenatal care, and the pregnancy was uncomplicated. The patient’s anatomy ultrasound at 20 weeks of gestation was unremarkable. The patient’s mother denies any family history of genetic diseases. The patient’s Apgar scores were notable for poor muscle tone at both one and five minutes of life. The patient’s birth weight is 2.6 kg (5 lb 11 oz), which is at the 5th percentile. His height and head circumference are in the 15th and 3rd percentile, respectively. On physical exam, the patient has a wide nasal bridge, downslanting palpebral fissures, and widely spaced eyes. He has good respiratory effort with a high-pitched cry. This patient is most likely to have experienced a deletion on which of the following chromosomes?
A 3-year-old boy presents to a geneticist for generalized developmental delay. Upon presentation he is found to have a distinctive facial structure with prominent epicanthal folds and macroglossia. Further physical examination reveals a simian crease on his palms bilaterally. Based on these findings, the physician strongly suspects Down syndrome and obtains a karyotype. Surprisingly the karyotype shows 46 chromosomes with two normal appearing alleles of chromosome 21. Further examination with fluorescent probes reveals a third copy of chromosome 21 genes that have been incorporated into another chromosome. What is the name of this mechanism of Down syndrome inheritance?
A 3500-g (7 lb 11 oz) healthy female newborn is delivered at 38 weeks' gestation. Chorionic villus sampling (CVS) in the first trimester showed a trisomy of chromosome 21 but the pregnancy was otherwise uncomplicated. Physical examination of the newborn is normal. Chromosomal analysis at birth shows a 46, XX karyotype. Which of the following is the most likely explanation for the prenatal chromosomal abnormality?
A 10-year-old boy is brought to a pediatrician by his mother for evaluation of fever, malaise, and rash with severe itching all over his body for the past 5 days. His immunization history is unavailable. His vital signs include: pulse 110/min, temperature 37.8°C (100.0°F), and respiratory rate 26/min. On examination of the skin, diffuse peeling vesicular lesions involving the arms and chest are observed. The pediatrician diagnoses the boy with chickenpox and reassures the mother. A few days later the boy returns to the clinic for a follow-up with his mother. The skin lesions have healed and there are scars. The formation of these scars is best described by which of the following statements?
A 62-year-old woman with type 2 diabetes mellitus comes to the physician because of a 1-year history of progressively worsening paresthesias in her upper limbs. She has accidentally burned her fingers on hot dishes several times. She was involved in a motor vehicle collision 3 years ago. Neurologic examination shows absent temperature sensation with normal fine touch sensation over the upper extremities and chest. Without treatment, this patient is at increased risk of developing which of the following?
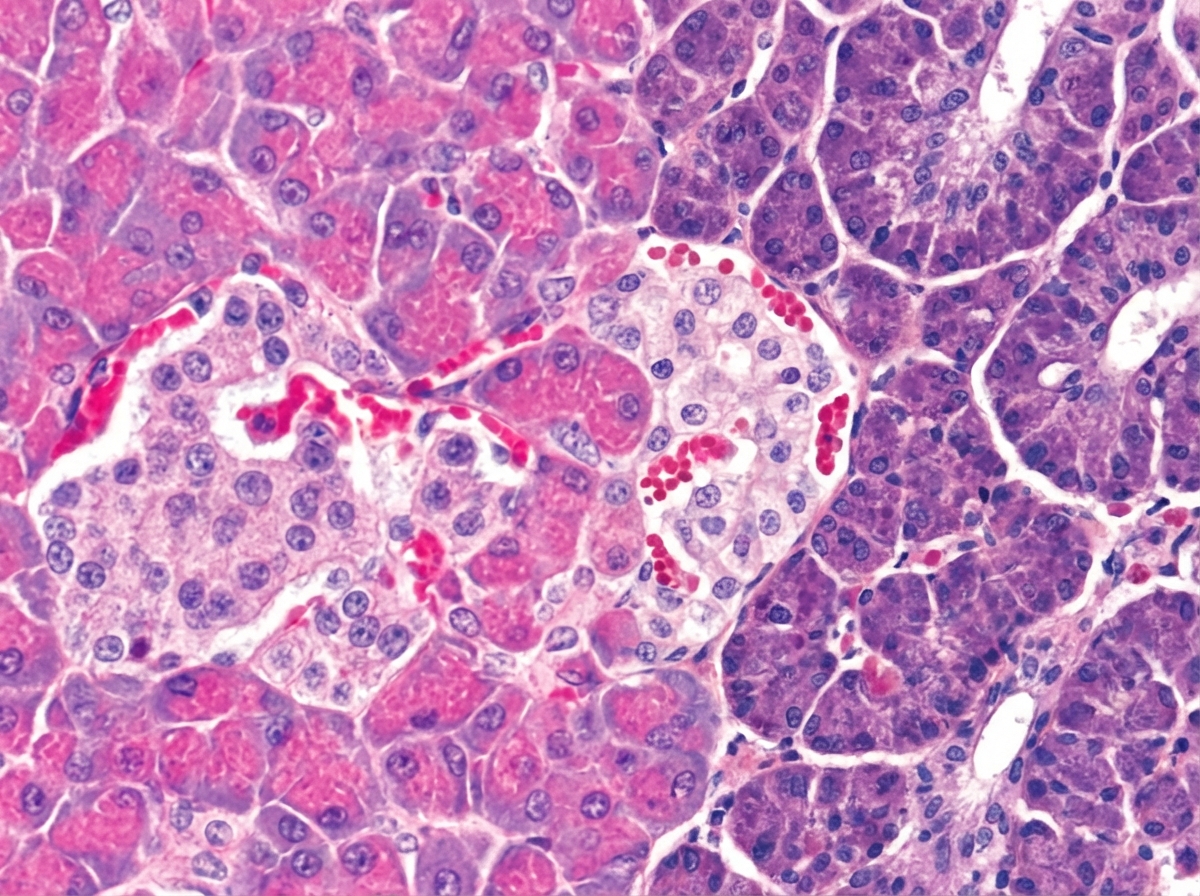
A pathologist examines a tissue specimen in which cells are grouped together in acini with visible ducts between them. He finds a patch of pale cells with a rich blood supply among the highly basophilic and granular cells. A representative micrograph is shown in the image. Which statement is correct about these cells?
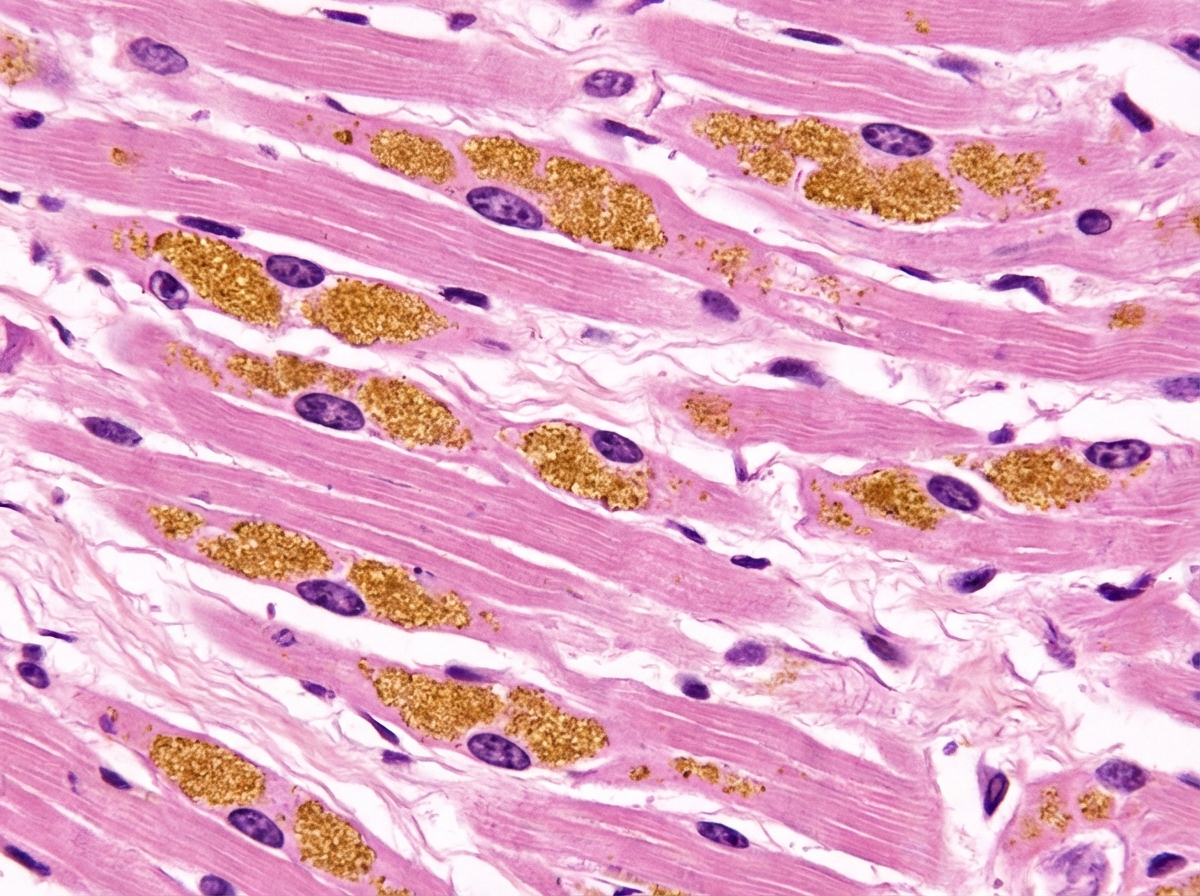
An 80-year-old male is found dead at home and brought in for an autopsy. The patient's heart shows a diminished ventricular chamber volume and the interventricular septum appears sigmoid shaped. The left atrium appears enlarged as well. A few calcifications are seen on the undamaged aortic valves. Microscopic examination reveals increased connective tissue in the myocardium and brown perinuclear cytoplasmic granules in numerous myocardial cells as shown in the exhibit. Which of the following most likely explains this patient's cardiac findings?
An 80-year-old woman is brought to the physician by her 2 daughters for worsening memory loss. They report that their mother is increasingly forgetful about recent conversations and events. She is unable to remember her appointments and commitments she has made. 3 years ago, the patient was moved into an elder care facility because she was often getting lost on her way home and forgetting to take her medications. The patient reports that she is very socially active at her new home and has long conversations with the other residents about her adventures as an air hostess during her youth. Which of the following cerebral pathologies is most likely present in this patient?
Practice by Chapter
Hemodynamic disorders
Practice Questions
Thromboembolic disease
Practice Questions
Shock pathophysiology
Practice Questions
Edema mechanisms
Practice Questions
Amyloidosis
Practice Questions
Genetic disorders
Practice Questions
Environmental pathology
Practice Questions
Nutritional diseases
Practice Questions
Pediatric pathology principles
Practice Questions
Forensic pathology principles
Practice Questions
Laboratory techniques in pathology
Practice Questions
Molecular diagnostic methods
Practice Questions
Immunohistochemistry
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app