
General Pathology — MCQs

On this page
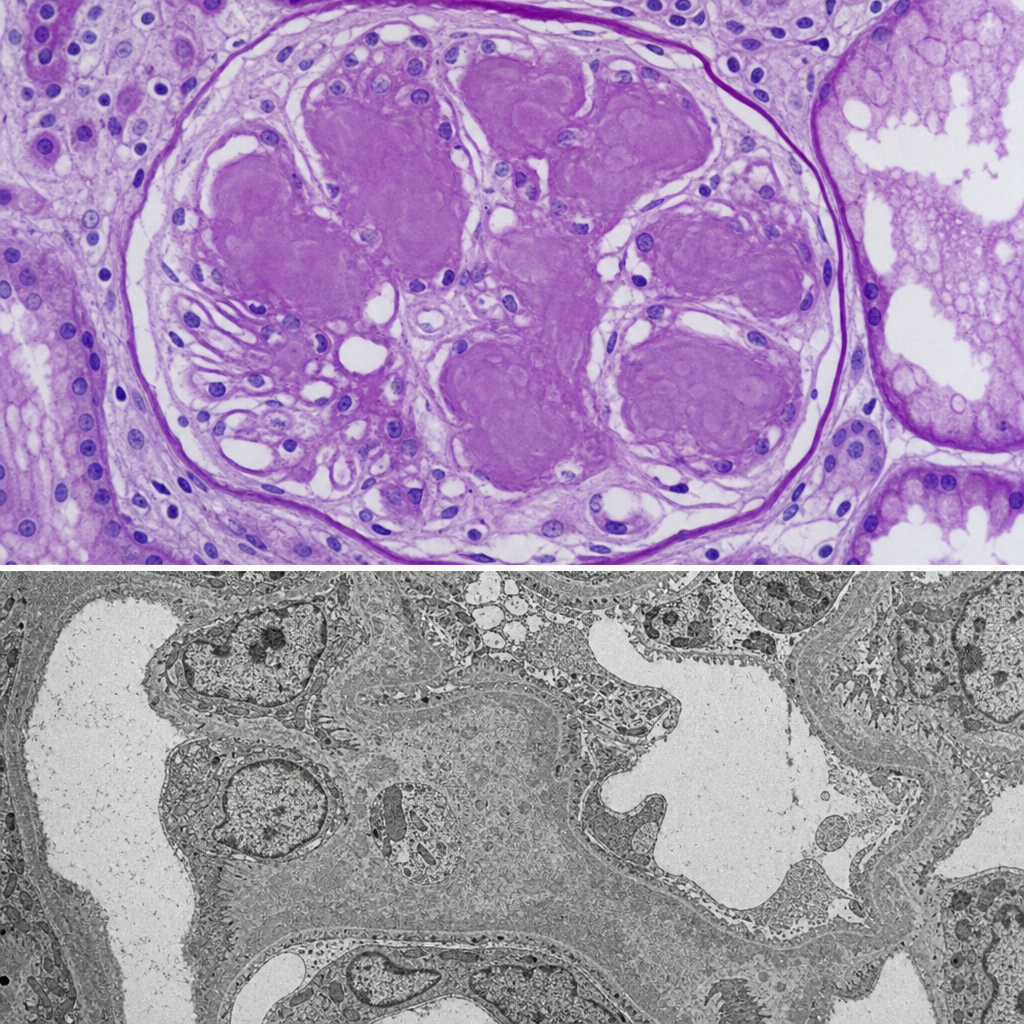
A 62-year-old man with a 20-year history of poorly controlled type 2 diabetes mellitus undergoes renal biopsy for progressive proteinuria and declining GFR. The photomicrograph shows glomeruli with periodic acid-Schiff (PAS)-positive, homogeneous, ovoid deposits in the mesangium that compress the glomerular capillaries; the deposits are acellular and do not stain with Congo red. Electron microscopy shows increased mesangial matrix without electron-dense deposits. Which of the following mechanisms is most directly responsible for the formation of the lesions seen in this biopsy?
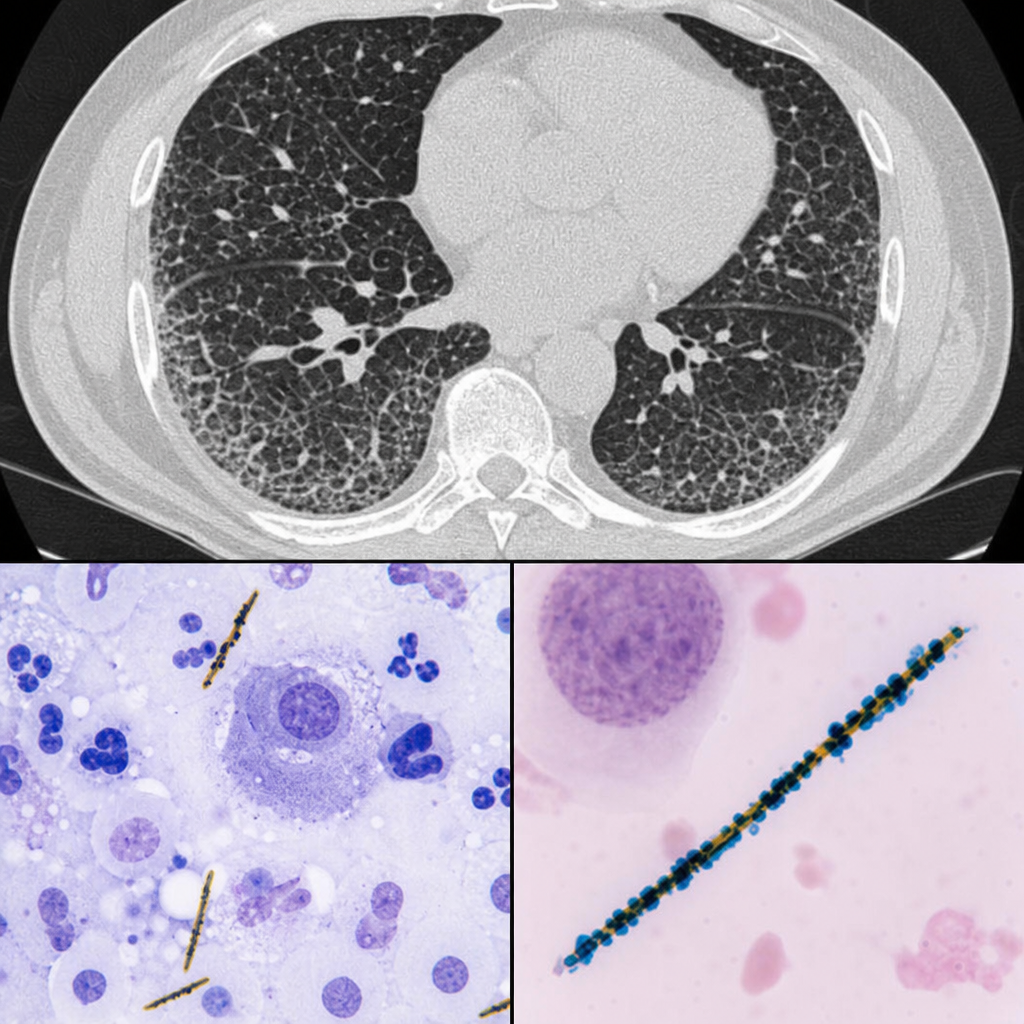
A 58-year-old man with a 40-pack-year smoking history presents with progressive dyspnea and a dry cough. Chest CT reveals bilateral lower lobe interstitial infiltrates. Bronchoalveolar lavage is performed. Prussian blue staining of the lavage material reveals elongated structures with a beaded, golden-brown coating. Which of the following is the most likely mechanism by which these structures form?
A 35-year-old woman with no significant past medical, past surgical, family or social history presents to clinic with a recently identified area of flat, intact, pigmented skin. The patient believes that this is a large freckle, and she states that it becomes darker during the summer when she is outdoors. On physical examination, you measure the lesion to be 6 mm in diameter. Which of the following is the best descriptor of this patient’s skin finding?
A 68-year-old male is brought to his primary care physician by his wife who is concerned that the patient seems more confused and irritable than usual. Three months ago, she started noticing that he appeared confused while doing simple tasks and seemed to be off balance. He has fallen several times over that time period. She has also noticed that if he is startled by one of their grandchildren, his arm starts to twitch uncontrollably. His past medical history is notable for transient ischemic attacks, hypertension, and hyperlipidemia. He takes aspirin, enalapril, hydrochlorothiazide, and rosuvastatin. He has a 30 pack-year smoking history. His family history is notable for Alzheimer’s disease in his mother and maternal uncle. His temperature is 98.6°F (37°C), blood pressure is 130/70 mmHg, pulse is 95/min, and respirations are 16/min. Physical examination reveals dysmetria and an ataxic gait. This patient’s condition is most strongly associated with which of the following findings on brain autopsy?
A 21-year-old man comes to the physician because of painful, firm, dark bumps on his neck and jawline. He has no history of serious illness and takes no medications. His brother had a similar rash. A photograph of the rash is shown. Which of the following is the most likely underlying mechanism of this patient's condition?

Two weeks after undergoing low anterior resection for rectal cancer, a 52-year-old man comes to the physician because of swelling in both feet. He has not had any fever, chills, or shortness of breath. His temperature is 36°C (96.8°F) and pulse is 88/min. Physical examination shows a normal thyroid and no jugular venous distention. Examination of the lower extremities shows bilateral non-pitting edema that extends from the feet to the lower thigh, with deep flexion creases. His skin is warm and dry, and there is no erythema or rash. Microscopic examination of the interstitial space in this patient's lower extremities would be most likely to show the presence of which of the following?
A 35-year-old nulligravid woman and her 33-year-old husband come to the physician for genetic counseling prior to conception. The husband has had severe psoriasis since adolescence that is now well-controlled under combination treatment with UV light therapy and etanercept. His father and two brothers also have this condition, and the couple wants to know how likely it is that their child will have psoriasis. The inheritance pattern of this patient's illness is most similar to which of the following conditions?
A 5-year-old girl accompanied by her mother presents to the emergency department after suffering a fall on the elementary school playground. Her mother reports that a child on the playground pushed her daughter who fell on her right side, after which she screamed and was found clutching her right leg. The girl's past medical history is significant for a fracture of the left femur and right radius over the past 2 years and an auditory deficit requiring hearing aid use starting 6 months ago. Inspection reveals a relatively short girl in moderate distress. She has brown opalescent teeth. She refuses to bear weight on her right lower extremity. Radiography of the right lower extremity reveals a femoral midshaft fracture. Which of the following is the most likely etiology of the patient's condition?
An investigator is attempting to develop a blood test to diagnose sporadic Creutzfeldt-Jakob disease (CJD). She has collected several tissue samples from adults who were diagnosed with CJD. After performing a comprehensive tissue analysis, she has identified two amino acid sequences on the affected proteins that are highly consistent across samples. She then creates antibodies that are highly specific to those amino acid sequences and is interested in using those antibodies to identify similar sequences in individuals suspected of having CJD. Which of the following tests would be most helpful in identifying these individuals?
A 48-year-old man is brought to the emergency department with a stab wound to his chest. The wound is treated in the emergency room. Three months later he develops a firm 4 x 3 cm nodular mass with intact epithelium over the site of the chest wound. On local examination, the scar is firm, non-tender, and there is no erythema. The mass is excised and microscopic examination reveals fibroblasts with plentiful collagen. Which of the following processes is most likely related to the series of events mentioned above?
Practice by Chapter
Hemodynamic disorders
Practice Questions
Thromboembolic disease
Practice Questions
Shock pathophysiology
Practice Questions
Edema mechanisms
Practice Questions
Amyloidosis
Practice Questions
Genetic disorders
Practice Questions
Environmental pathology
Practice Questions
Nutritional diseases
Practice Questions
Pediatric pathology principles
Practice Questions
Forensic pathology principles
Practice Questions
Laboratory techniques in pathology
Practice Questions
Molecular diagnostic methods
Practice Questions
Immunohistochemistry
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app