
Endocrine effects of non-endocrine tumors — MCQs

A 61-year-old man presents to the urgent care clinic complaining of cough and unintentional weight loss over the past 3 months. He works as a computer engineer, and he informs you that he has been having to meet several deadlines recently and has been under significant stress. His medical history is significant for gout, hypertension, hypercholesterolemia, diabetes mellitus type 2, and pulmonary histoplasmosis 10 years ago. He currently smokes 2 packs of cigarettes/day, drinks a 6-pack of beer/day, and he endorses a past history of cocaine use back in the early 2000s but currently denies any drug use. The vital signs include: temperature 36.7°C (98.0°F), blood pressure 126/74 mm Hg, heart rate 87/min, and respiratory rate 18/min. His physical examination shows minimal bibasilar rales, but otherwise clear lungs on auscultation, grade 2/6 holosystolic murmur, and a benign abdominal physical examination. However, on routine lab testing, you notice that his sodium is 127 mEq/L. His chest X-ray is shown in the picture. Which of the following is the most likely underlying diagnosis?

A 54-year-old man comes to the emergency department because of abdominal distension for the past 3 weeks. He also complains of generalized abdominal discomfort associated with nausea and decreased appetite. He was discharged from the hospital 3 months ago after an inguinal hernia repair with no reported complications. He has a history of type 2 diabetes mellitus, congestive heart failure, and untreated hepatitis C. His current medications include aspirin, atorvastatin, metoprolol, lisinopril, and metformin. His father has a history of alcoholic liver disease. He has smoked one pack of cigarettes daily for 30 years but quit 5 years ago. He drinks 3–4 beers daily. He appears cachectic. His vital signs are within normal limits. Examination shows a distended abdomen and shifting dullness. There is no abdominal tenderness or palpable masses. There is a well-healed surgical scar in the right lower quadrant. Examination of the heart and lung shows no abnormalities. He has 1+ bilateral lower extremity nonpitting edema. Diagnostic paracentesis is performed. Laboratory studies show: Hemoglobin 10 g/dL Leukocyte count 14,000/mm3 Platelet count 152,000/mm3 Serum Total protein 5.8 g/dL Albumin 3.5 g/dL AST 18 U/L ALT 19 U/L Total bilirubin 0.8 mg/dL HbA1c 8.1% Peritoneal fluid analysis Color Cloudy Cell count 550/mm3 with lymphocytic predominance Total protein 3.5 g/dL Albumin 2.6 g/dL Glucose 60 mg/dL Triglycerides 360 mg/dL Peritoneal fluid Gram stain is negative. Culture and cytology results are pending. Which of the following is the most likely cause of this patient's symptoms?
A 70-year-old male is brought to the emergency department from a nursing home due to worsening mental status. His nurse reports that the patient has been very lethargic and sleeping more than usual for the past week. She found him confused and difficult to arouse this morning and decided to bring him to the ER. His past medical history is significant for small cell carcinoma of the lung for which he is receiving chemotherapy. He is also on lithium and bupropion for bipolar disorder. Other medications include metoprolol, valsartan, metformin, and insulin. On admission, blood pressure is 130/70 mm Hg, pulse rate is 100/min, respiratory rate is 17/min, and temperature is 36.5°C (97.7°F). He is drowsy and disoriented. Physical examination is normal. Finger-stick glucose level is 110 mg/dL. Other laboratory studies show: Na+ 120 mEq/L (136—145 mEq/L) K+ 3.5 mEq/L (3.5—5.0 mEq/L) Cl- 107 mEq/L (95—105 mEq/L) Creatinine 0.8 mg/dL (0.6—1.2 mg/dL) Serum osmolality 250 mOsm/kg (275—295 mOsm/kg) Urine Na+ 70 mEq/L Urine osmolality 340 mOsm/kg He is admitted to the hospital for further management. Which of the following is the most likely cause of this patient's condition?
A 75-year-old gentleman is brought to the ED with confusion that started earlier this morning. His family notes that he was complaining of feeling weak last night and also had a slight tremor at the time. He is afebrile and he has no known chronic medical conditions. Physical exam reveals a cooperative but confused gentleman. His mucous membranes are moist, he has no focal neurological deficits, and his skin turgor is within normal limits. His lab results are notable for: Serum Na+: 123 mEq/L Plasma osmolality: 268 mOsm/kg Urine osmolality: 349 mOsm/kg Urine Na+: 47 mEq/L Which of the following malignancies is most likely to be responsible for this patient's presentation?
A 65-year-old man comes to the physician for evaluation of a neck mass and weight loss. He first noticed the growing mass 2 months ago. The mass is not painful. He also has decreased appetite and intermittent abdominal pain. He has lost 10 kg (22 lb) of weight over the past 3 months. Sometimes, he wakes up in the morning drenched in sweat. He takes daily over-the-counter multivitamins. He appears pale. His pulse is 65/min, blood pressure is 110/70 mm Hg, and temperature is 38.1°C (100.6°F). Physical exam shows a painless, golf ball-sized mass in the anterior triangle of the neck. A biopsy shows large cells with a bilobed nucleus that are CD15-positive and CD30-positive. Laboratory analysis of serum shows a calcium level of 14.5 mg/dL and a parathyroid hormone level of 40 pg/mL. Which of the following is the most likely explanation of this patient's laboratory findings?
A lung mass of a 50 pack-year smoker is biopsied. If ADH levels were grossly increased, what would most likely be the histologic appearance of this mass?
A 38-year-old female presents to her primary care physician with complaints of several episodes of palpitations accompanied by panic attacks over the last month. She also is concerned about many instances over the past few weeks where food has been getting stuck in her throat and she has had trouble swallowing. She denies any prior medical problems and reports a family history of cancer in her mother and maternal grandfather but cannot recall any details regarding the type of cancer(s) or age of diagnosis. Her vital signs at today's visit are as follows: T 37.6 deg C, HR 106, BP 158/104, RR 16, SpO2 97%. Physical examination is significant for a nodule on the anterior portion of the neck that moves with swallowing, accompanied by mild lymphadenopathy. A preliminary work-up is initiated, which shows hypercalcemia, elevated baseline calcitonin, and an inappropriately elevated PTH level. Diagnostic imaging shows bilateral adrenal lesions on an MRI of the abdomen/pelvis. Which of the following is the most likely diagnosis in this patient?
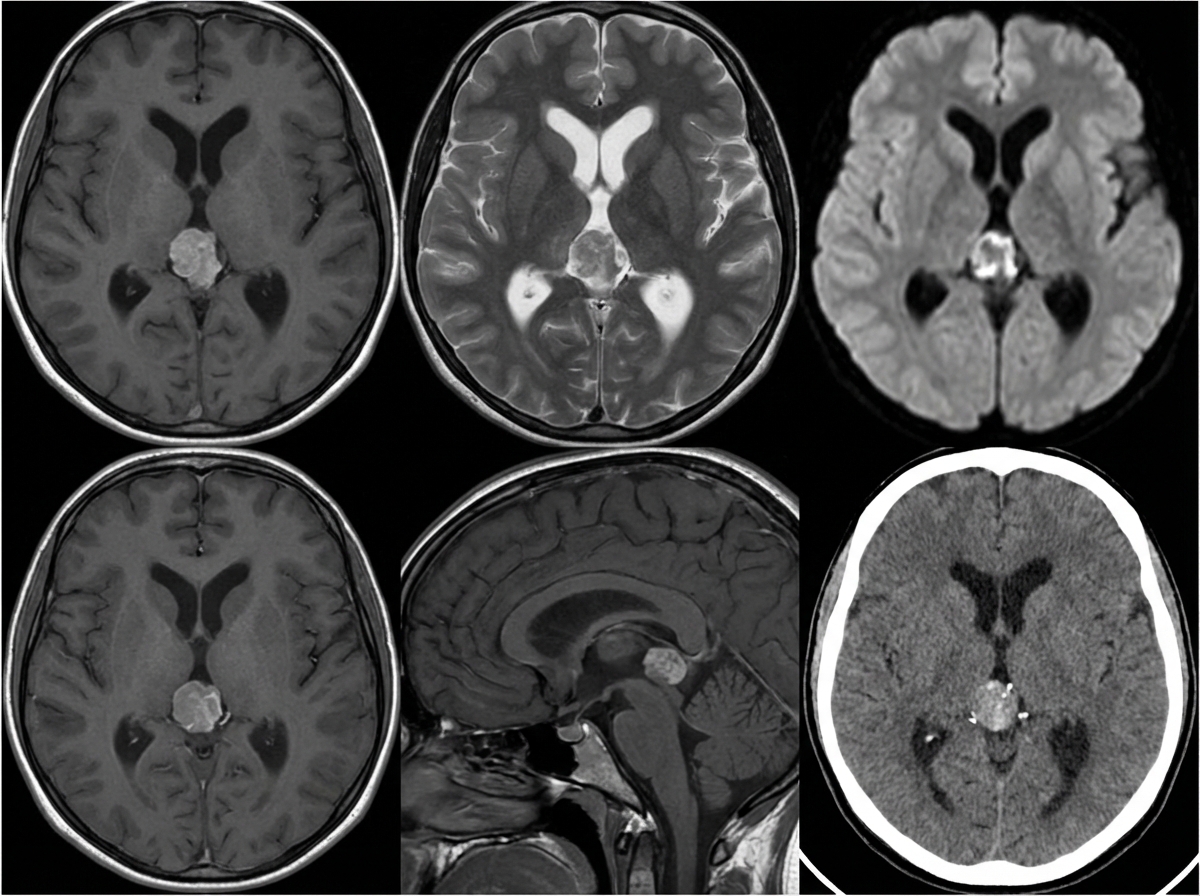
A 10-year-old girl is brought to the physician by her parents due to 2 months of a progressively worsening headache. The headaches were initially infrequent and her parents attributed them to stress from a recent move. However, over the last week the headaches have gotten significantly worse and she had one episode of vomiting this morning when she woke up. Her medical history is remarkable for a hospitalization during infancy for bacterial meningitis. On physical exam, the patient has difficulty looking up. The lower portion of her pupil is covered by the lower eyelid and there is sclera visible below the upper eyelid. A magnetic resonance imaging (MRI) of the brain is shown. Which of the following is the most likely diagnosis?
A 40-year-old man presents with a painless firm mass in the right breast. Examination shows retraction of the nipple and the skin is fixed to the underlying mass. The axillary nodes are palpable. Which of the following statements is FALSE regarding the above condition?
A neurophysiologist describes the mechanism of a specific type of synaptic transmission to his students. While illustrating this, he points out that when the action potential reaches the presynaptic terminal of a chemical synapse, the voltage-gated Ca2+ channels open. Ca2+ ions trigger the release of neurotransmitters from vesicles in the presynaptic terminal. In this type of synaptic transmission, increased cytosolic Ca2+ levels cause the release of a neurotransmitter from small vesicles with dense cores. Which of the following neurotransmitters is most likely to be the one that is released into the synaptic cleft in this type of synapse?
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app