
Vesiculobullous diseases — MCQs

A 64-year-old man presents to his primary care provider after noticing the development of a blistering rash. The patient states that his symptoms began 1 week ago after he noticed a blister develop on the inside of his mouth that eventually ruptured. Over the past several days, he has noticed several more blisters on his torso. The patient denies a fever or any other symptoms. He has a history of high blood pressure, for which he takes hydrochlorothiazide. He is otherwise healthy and denies any recent changes to his medication. Today, the patient’s temperature is 99.0°F (37.2°C), blood pressure is 124/84 mmHg, pulse is 66/min, and respirations are 12/min. On exam, the patient’s mouth is notable for a previously ruptured blister on his left buccal mucosa. On his left flank and anterior abdomen are scattered 10-15-cm bullae that appear flaccid and filled with serous fluid. The lesions are erythematous but there is no surrounding erythema. On manual rubbing of the skin near the lesions, new blisters form within minutes. Which of the following is involved in the pathogenesis of this disease?
A 50-year-old woman comes to the physician because of blisters on her forearm that appeared 3 days ago. She also reports pain in her left cheek when eating and pain during sexual intercourse for the past week. She has not been sick for the past 6 months. She has started hiking in the woods on the weekends with her son a couple months ago but has been careful to avoid poison ivy. She has a history of hypertension and osteoarthritis. She recently started taking captopril and stopped taking meloxicam 2 weeks ago. She has a family history of pernicious anemia and Graves' disease. The patient's vital signs are within normal limits. Examination reveals multiple, flaccid blisters on the volar surface of the forearm and ulcers on the buccal, gingival, and vulvar mucosa. The epidermis on the forearm separates when the skin is lightly stroked. The total body surface area involvement of the blisters is estimated to be 10%. The remainder of the examination shows no abnormalities. Which of the following is the most likely diagnosis?
A 22-year-old woman presents to the emergency department with a 2-day history of severe blistering. She says that she woke up 2 days ago with a number of painful blisters in her mouth and has since been continuing to develop blisters of her cutaneous skin all over her body and the mucosa of her mouth. She has no past medical history and has never experienced these symptoms before. Physical exam reveals a diffuse vesicular rash with painful, flaccid blisters that separate easily with gentle rubbing. The function of which of the following proteins is most likely disrupted in this patient?
A 45-year-old man visits the office with complaints of severe pain with urination for 5 days. In addition, he reports having burning discomfort and itchiness at the tip of his penis. He is also concerned regarding a yellow-colored urethral discharge that started a week ago. Before his symptoms began, he states that he had sexual intercourse with multiple partners at different parties organized by the hotel he was staying at. Physical examination shows edema and erythema concentrated around the urethral meatus accompanied by a mucopurulent discharge. Which of the following diagnostic tools will best aid in the identification of the causative agent for his symptoms?
A 58-year-old woman presents with tense bullae on an erythematous base, primarily affecting her trunk and extremities. The lesions developed over the past 3 weeks. Nikolsky sign is negative. Skin biopsy shows subepidermal bullae with eosinophilic infiltrate. Direct immunofluorescence shows linear deposits of IgG and C3 at the basement membrane zone. Which of the following is the target antigen in this condition?
A 53-year-old woman seeks medical care for superficial erosions and blisters over the skin of her head and trunk. She also has significant involvement of her buccal mucosa, which has made eating difficult. A year earlier, she developed tender sores on the oral mucosa and soft palate of her mouth, which was initially treated as herpes simplex stomatitis. Her condition worsened despite treatment, resulting in the development of eroded areas over her trunk and extremities, with a 10 kg weight loss. Upon further questioning, she denies itching, but she notes that the top layer of her skin could be easily removed when firm horizontal pressure was applied. What is the most likely diagnosis for this patient’s condition?
A 54-year-old man comes to the physician because of a cough with blood-tinged sputum for 1 week. He also reports fever and a 5-kg (11 lb) weight loss during the past 2 months. Over the past year, he has had 4 episodes of sinusitis. Physical examination shows palpable nonblanching skin lesions over the hands and feet. Examination of the nasal cavity shows ulceration of the nasopharyngeal mucosa and a depressed nasal bridge. Oral examination shows a painful erythematous gingival enlargement that bleeds easily on contact. Which of the following is the most likely cause of the patient's symptoms?
A 72-year-old nursing home resident is complaining of pruritis. She is noted to have multiple, tense blisters on her trunk as well as the flexor surfaces of her extremities. The blisters have an erythematous base. You are unable to extend the blisters when you apply lateral traction. You suspect an autoimmune bullous dermatosis. Which of the following is the cause of the likely condition?
You are seeing an otherwise healthy 66-year-old male in clinic who is complaining of localized back pain and a new rash. On physical exam, his vital signs are within normal limits. You note a vesicular rash restricted to the upper left side of his back. In order to confirm your suspected diagnosis, you perform a diagnostic test. What would you expect to find on the diagnostic test that was performed?
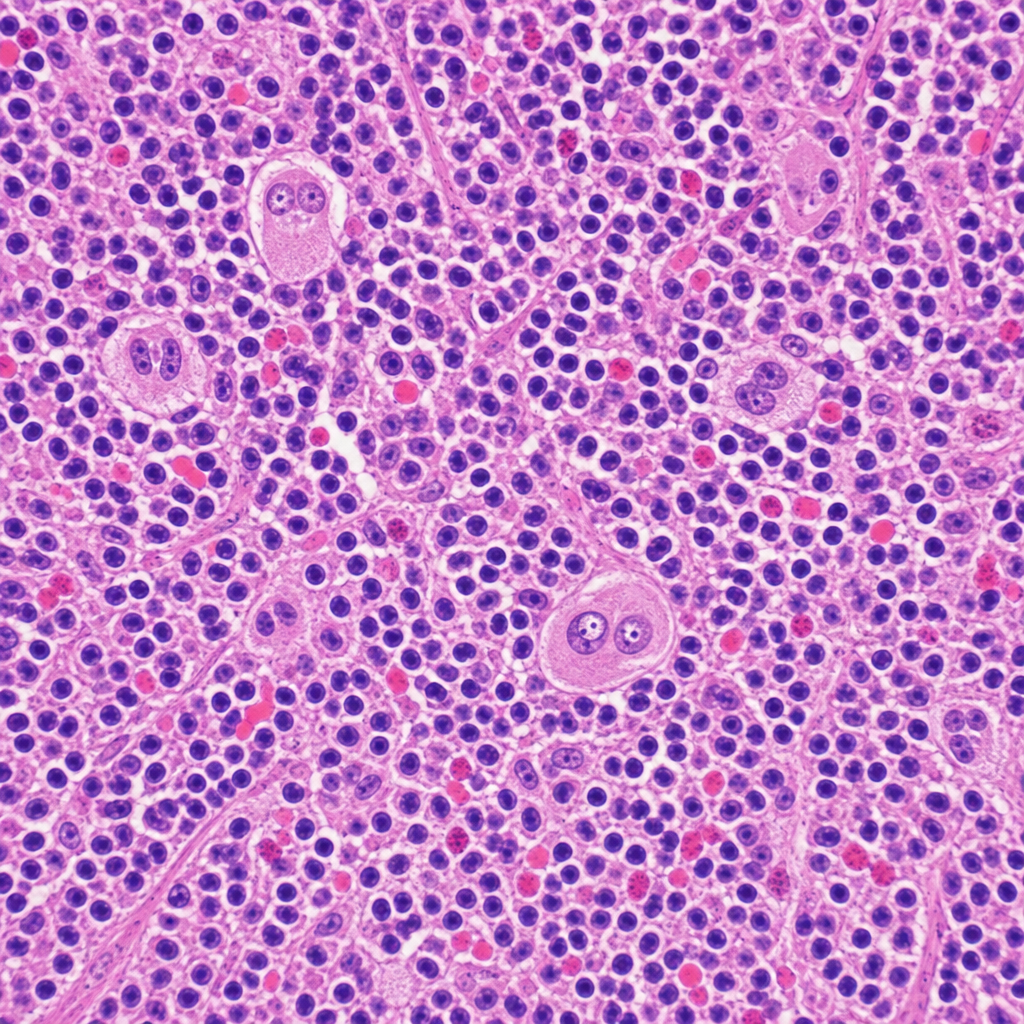
A 34-year-old woman presents with fatigue, night sweats, and a painless cervical lymph node mass for 3 months. Excisional biopsy of the lymph node is performed. The photomicrograph demonstrates a mixed cellular infiltrate with scattered large binucleated cells possessing prominent eosinophilic 'owl-eye' nucleoli, set against a background of lymphocytes, plasma cells, eosinophils, and fibroblasts. Immunohistochemical staining of the large cells is positive for CD15 and CD30 and negative for CD45. Which of the following best describes the cell of origin of the large binucleated cells seen in this lesion?
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app