
Dermatopathology — MCQs

On this page
A 55-year-old farmer presents with a 2-year history of a slowly growing nodule on his nose with rolled borders and central ulceration. Biopsy shows nests of basaloid cells with peripheral palisading extending from the epidermis into the dermis, surrounded by stromal retraction. Mitoses are present but not prominent. Apply this pathological finding to determine appropriate management.
A 28-year-old man with a history of recurrent staphylococcal abscesses presents with multiple painful nodules in the axillae and groin that drain purulent material. Biopsy shows dilated follicles with keratinous plugging, mixed inflammatory infiltrate with neutrophils, and sinus tract formation extending into the subcutaneous tissue. Apply this information to guide management.
A 45-year-old woman presents with a pruritic rash on her wrists and ankles. Physical examination reveals flat-topped, polygonal, violaceous papules with white striae on their surface. Skin biopsy shows a dense band-like lymphocytic infiltrate at the dermal-epidermal junction with apoptotic keratinocytes and sawtooth rete ridges. Apply your knowledge to determine the most likely diagnosis.
The following skin biopsy from a patient of leprosy shows well-formed epithelioid granulomas extending close to the epidermis, with surrounding lymphocytes and no demonstrable acid-fast bacilli on Fite-Faraco staining. The biopsy is diagnostic of:
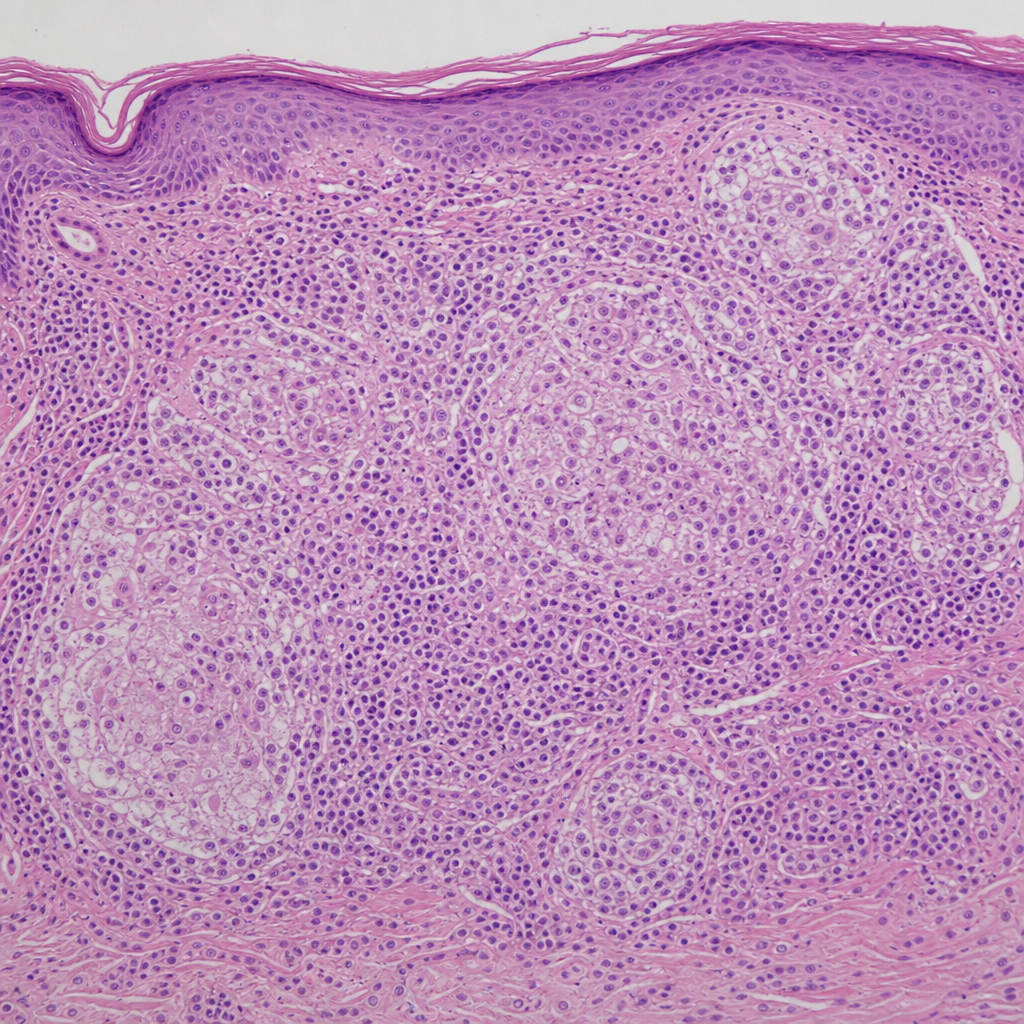
The following skin biopsy from a patient with leprosy is diagnostic of which form of the disease? (Recent NEET Pattern 2016-17) Fite-Faraco staining for acid-fast bacilli was negative.
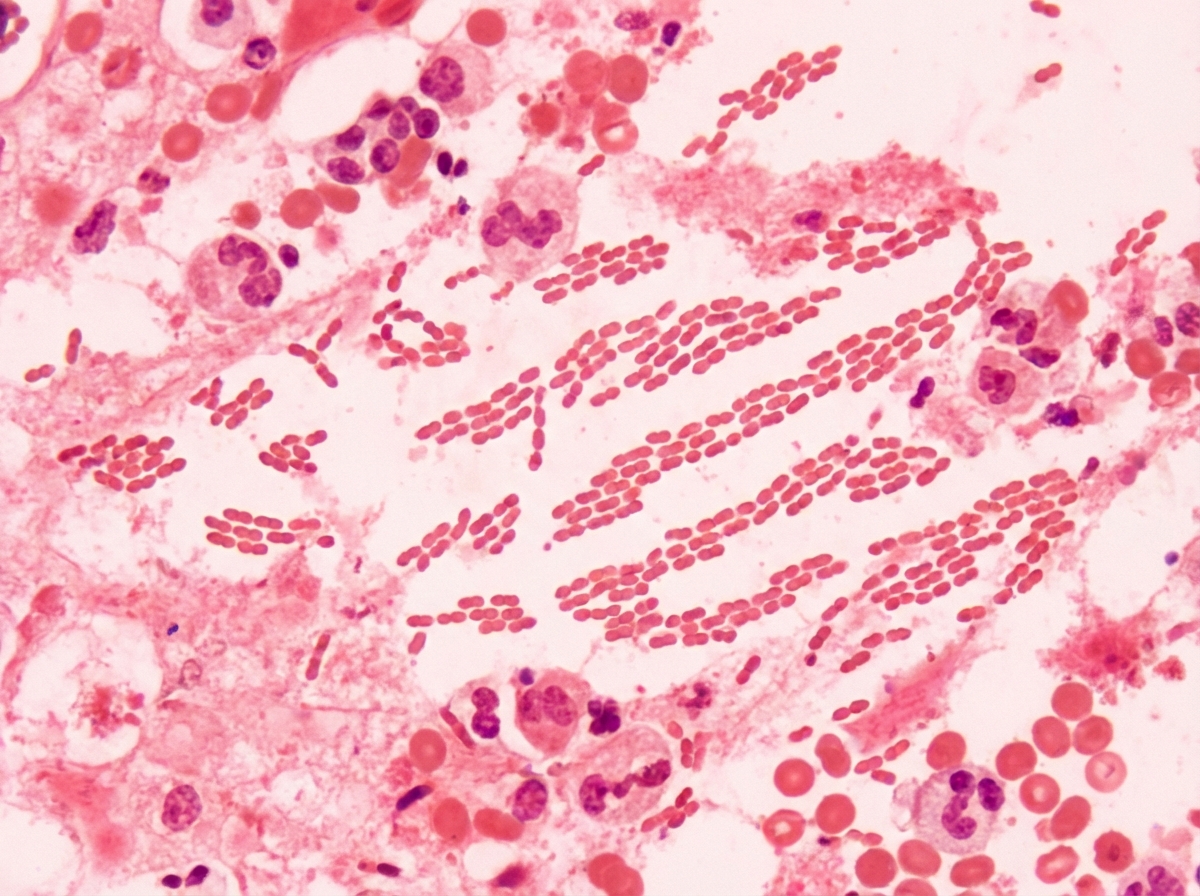
The following is a picture from scrapping of genital ulcer. Comment on the diagnosis. (AIIMS May 2017)
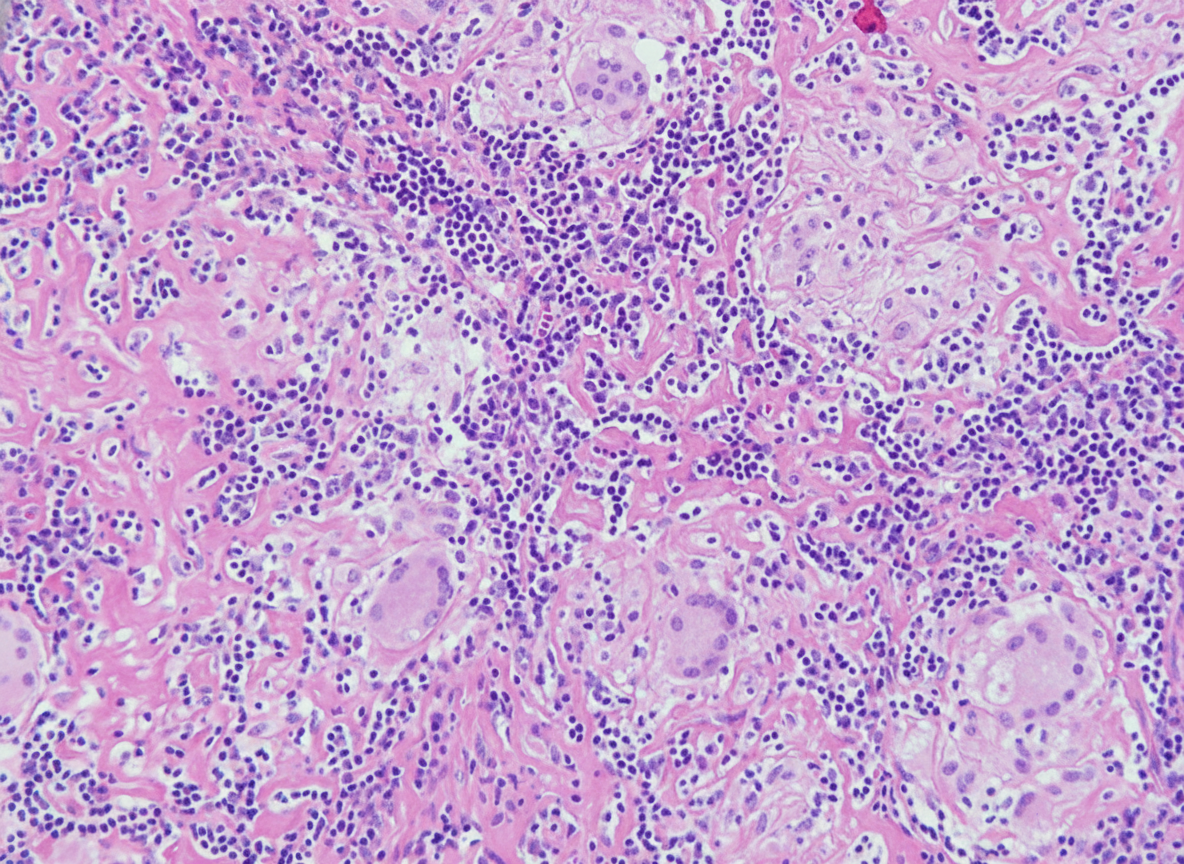
A 12-year-old boy develops multiple lumps in the skin. Biopsy of the lumps is shown below. What is the probable causative agent? (NEET Pattern 2019)
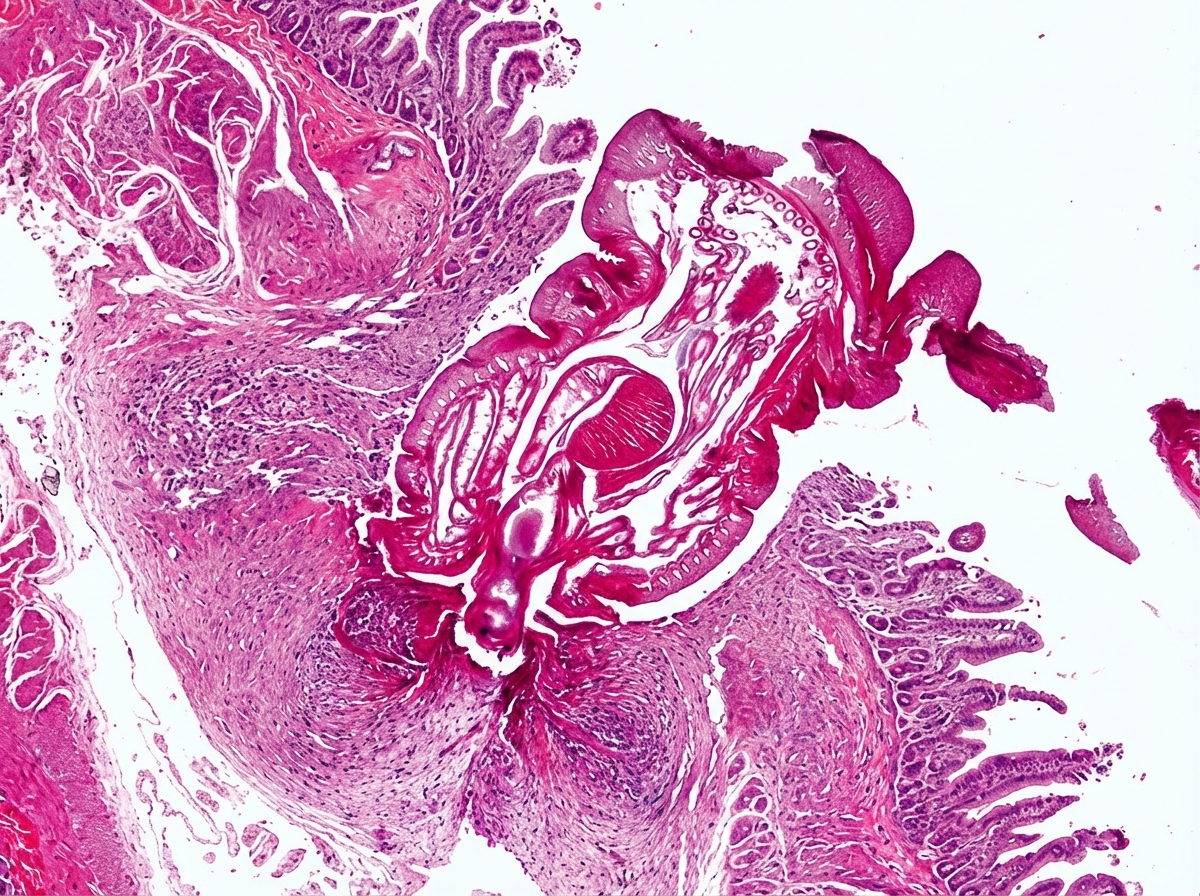
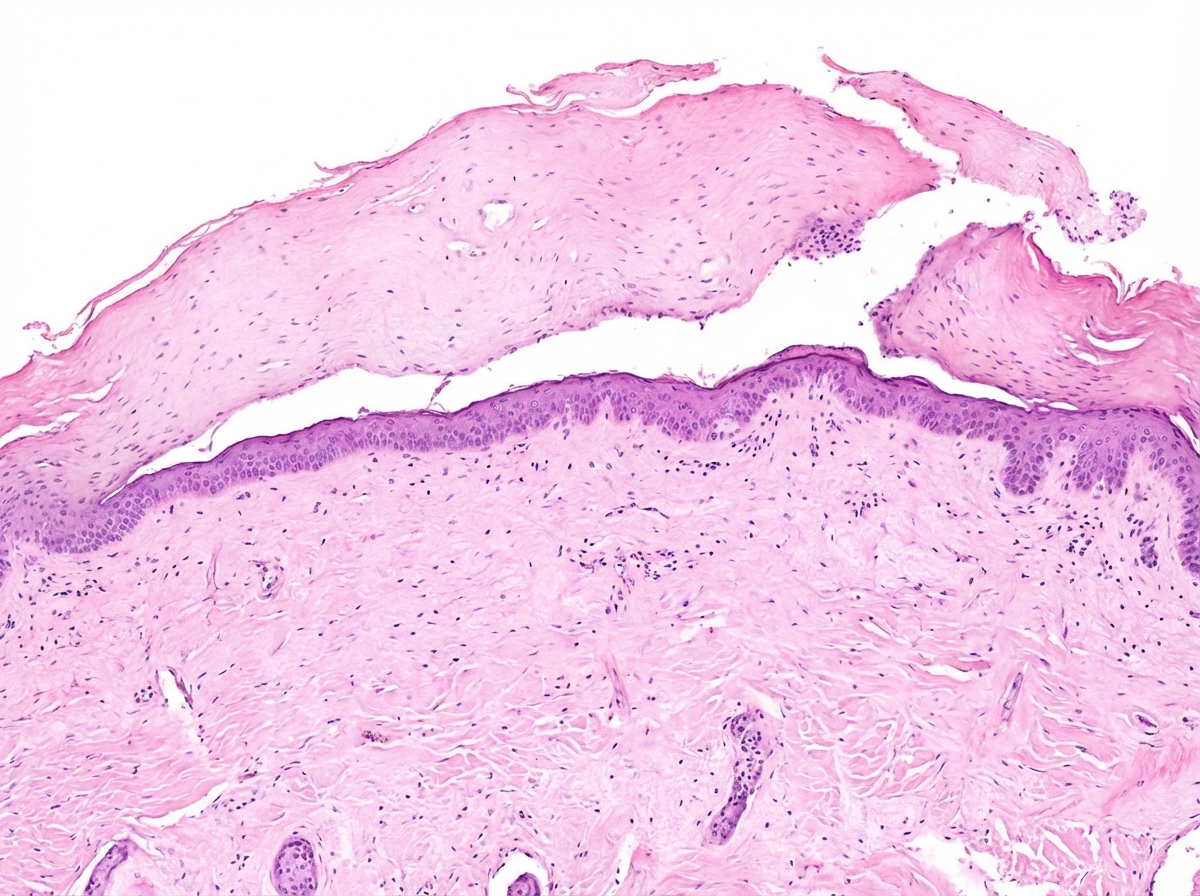
Identify the histopathological slide shown below:
Practice by Chapter
Inflammatory dermatoses
Practice Questions
Vesiculobullous diseases
Practice Questions
Infectious skin diseases
Practice Questions
Benign epithelial tumors
Practice Questions
Premalignant skin lesions
Practice Questions
Non-melanoma skin cancers
Practice Questions
Melanocytic nevi
Practice Questions
Melanoma pathology
Practice Questions
Adnexal tumors
Practice Questions
Dermal tumors and proliferations
Practice Questions
Panniculitis
Practice Questions
Vascular disorders of skin
Practice Questions
Disorders of pigmentation
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app