
Benign epithelial tumors — MCQs

A 23-year-old woman comes to the physician because of a 5-month history of a pruritic rash on the bilateral upper extremities. She has no history of serious illness and takes no medications. A skin biopsy of the rash shows intraepidermal accumulation of edematous fluid and widening of intercellular spaces between keratinocytes. Which of the following is the most likely diagnosis?
A 70-year-old man comes to the physician because of a painless skin lesion on his neck for the past 5 months. The lesion has gradually become darker in color and is often pruritic. He has a similar lesion on the back. He is a retired landscaper. He has smoked half a pack of cigarettes daily for 45 years. Physical examination shows a 0.9-cm hyperpigmented papule on the neck with a greasy, wax-like, and stuck-on appearance. Histopathologic examination is most likely to show which of the following?
A 65-year-old woman presents to a dermatology clinic complaining about a couple of well-demarcated, dark, round skin lesions on her face. She claims she has had these lesions for 3 or 4 years. The lesions are painless, not pruritic, and have never bled. However, she is moderately distressed about the potential malignancy of these lesions after she heard that a close friend was just diagnosed with a melanoma. The medical history is unremarkable. Physical examination reveals a few well-demarcated, round, verrucous lesions, with a stuck-on appearance, distributed on the patient's back and face (see image). Under a dermatoscope, the lesions showed multiple comedo-like openings, milia cysts, and a cerebriform pattern. What is the best next step of management?

A 66-year-old man presents to his family physician complaining of a sandpaper-like sensation when he touches the lesion on his forehead. His medical history is relevant for hypertension and hypercholesterolemia, for which he is taking losartan and atorvastatin. He used to work as a gardener, but he retired 3 years ago. His vital signs are within normal limits. Physical examination of his forehead reveals male-pattern baldness and thin, adherent, yellow-colored skin lesions that feel rough to the touch (see image). His family physician refers to him to a dermatologist for further management and treatment. Which of the following conditions would the patient most likely develop if this skin condition is left untreated?

A 43-year-old woman comes to the physician for an annual health maintenance examination. On questioning, she has had fatigue and headaches for the last month. A few weeks ago, she had to have her wedding ring resized because it had become too small for her finger. She has mild persistent asthma and anxiety disorder. She drinks 2–3 glasses of red wine per night and has smoked one pack of cigarettes daily for 16 years. She works a desk job in accounting and has recently been working long hours due to an upcoming company merger. Her father has a history of a pituitary adenoma. Current medications include alprazolam, a fluticasone inhaler, and an albuterol inhaler. She is 160 cm (5 ft 3 in) tall and weighs 81.6 kg (180 lb); her BMI is 32 kg/m2. Her temperature is 37.2°C (99°F), pulse is 92/min, and blood pressure is 132/80 mm Hg. Examination shows no abnormalities. Fasting laboratory studies show: Hemoglobin 13 g/dL Serum Na+ 135 mEq/L K+ 4.6 mEq/L Cl- 105 mEq/L HCO3- 22 mEq/L Urea nitrogen 17 mg/dL Glucose 160 mg/dL Creatinine 0.9 mg/dL Which of the following is the most likely underlying mechanism of this patient's hyperglycemia?
A 27-year-old G2P0A2 woman comes to the office complaining of light vaginal spotting. She received a suction curettage 2 weeks ago for an empty gestational sac. Pathology reports showed hyperplastic and hydropic trophoblastic villi, but no fetal tissue. The patient denies fever, abdominal pain, dysuria, dyspareunia, or abnormal vaginal discharge. She has no chronic medical conditions. Her periods are normally regular and last 3-4 days. One year ago, she had an ectopic pregnancy that was treated with methotrexate. She has a history of chlamydia and gonorrhea that was treated 5 years ago with azithromycin and ceftriaxone. Her temperature is 98°F (36.7°C), blood pressure is 125/71 mmHg, and pulse is 82/min. On examination, hair is present on the upper lip, chin, and forearms. A pelvic examination reveals a non-tender, 6-week-sized uterus and bilateral adnexal masses. There is scant dark blood in the vaginal vault on speculum exam. A quantitative beta-hCG is 101,005 mIU/mL. Two weeks ago, her beta-hCG was 63,200 mIU/mL. A pelvic ultrasound shows bilaterally enlarged ovaries with multiple thin-walled cysts between 2-3 cm in size. Which of the following is the most likely cause of the patient’s adnexal masses?
A 48-year-old man is brought to the emergency department with a stab wound to his chest. The wound is treated in the emergency room. Three months later he develops a firm 4 x 3 cm nodular mass with intact epithelium over the site of the chest wound. On local examination, the scar is firm, non-tender, and there is no erythema. The mass is excised and microscopic examination reveals fibroblasts with plentiful collagen. Which of the following processes is most likely related to the series of events mentioned above?
A 41-year-old male who takes NSAIDs regularly for his chronic back pain develops severe abdominal pain worse with eating. Upper endoscopy is performed and the medical student asks the supervising physician how the histological differentiation between a gastric ulcer and erosion is made. Which of the following layers of the gastric mucosa MUST be breached for a lesion to be considered an ulcer?
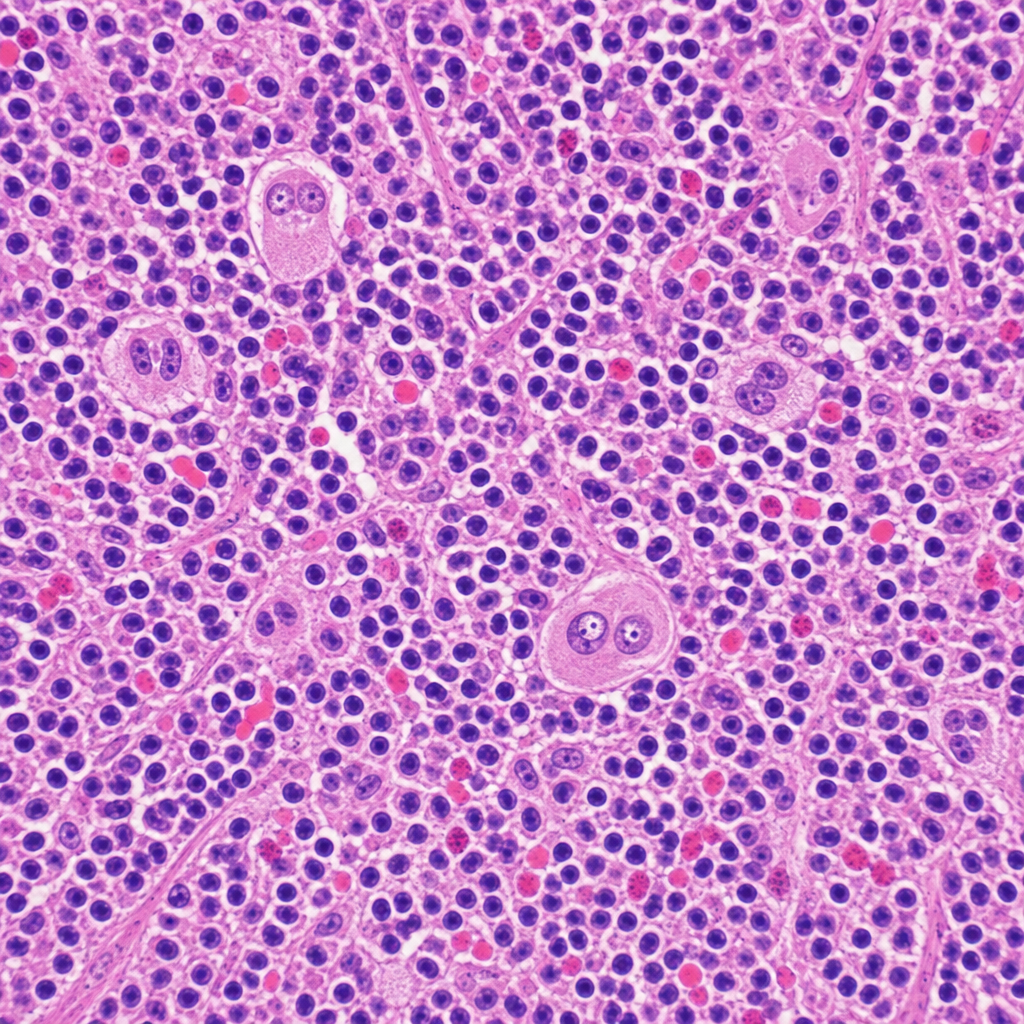
A 34-year-old woman presents with fatigue, night sweats, and a painless cervical lymph node mass for 3 months. Excisional biopsy of the lymph node is performed. The photomicrograph demonstrates a mixed cellular infiltrate with scattered large binucleated cells possessing prominent eosinophilic 'owl-eye' nucleoli, set against a background of lymphocytes, plasma cells, eosinophils, and fibroblasts. Immunohistochemical staining of the large cells is positive for CD15 and CD30 and negative for CD45. Which of the following best describes the cell of origin of the large binucleated cells seen in this lesion?
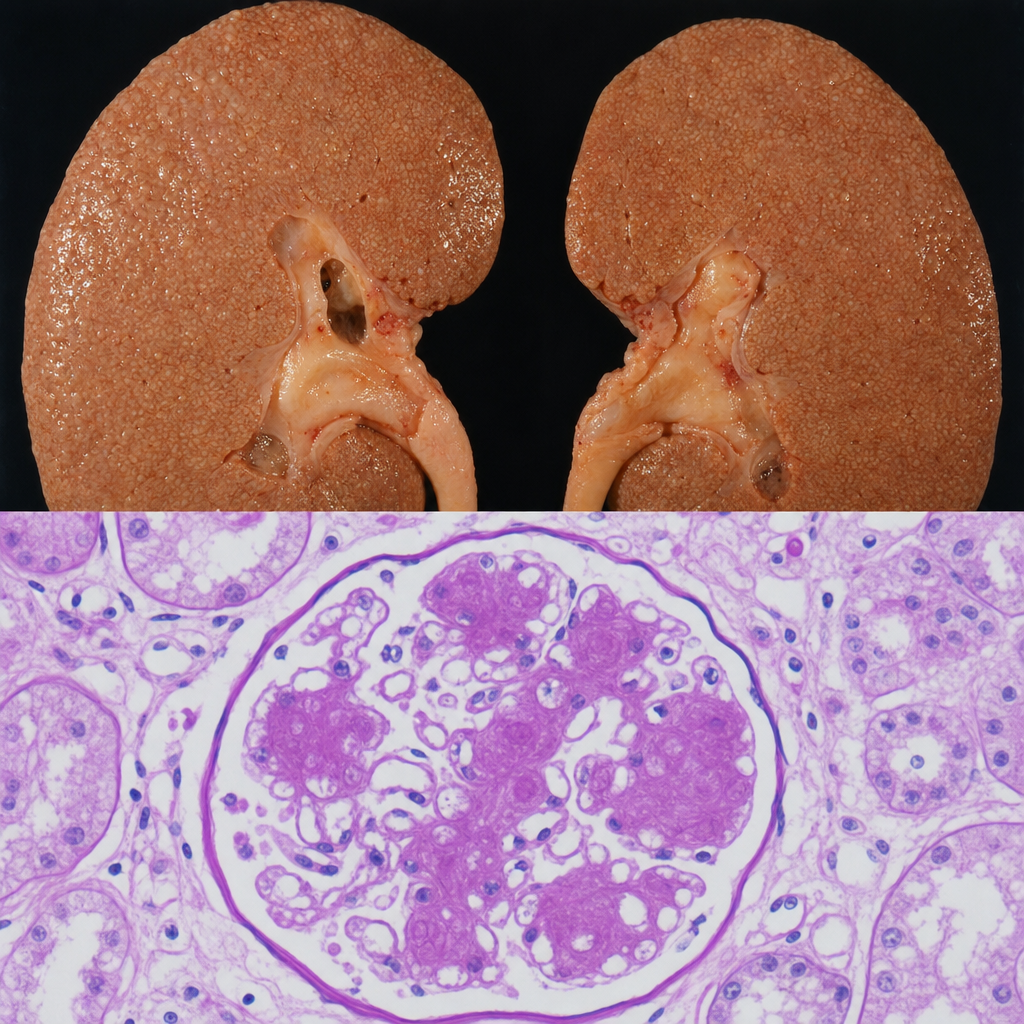
A 67-year-old man with a 20-year history of poorly controlled type 2 diabetes mellitus dies of a myocardial infarction. At autopsy, the kidneys are symmetrically enlarged with a granular cortical surface. PAS staining of the renal cortex shows PAS-positive ovoid deposits within the mesangium of glomeruli, compressing the adjacent capillary loops. Which of the following best describes the composition and pathogenetic mechanism of these deposits?
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app