
Dermatopathology — MCQs

On this page
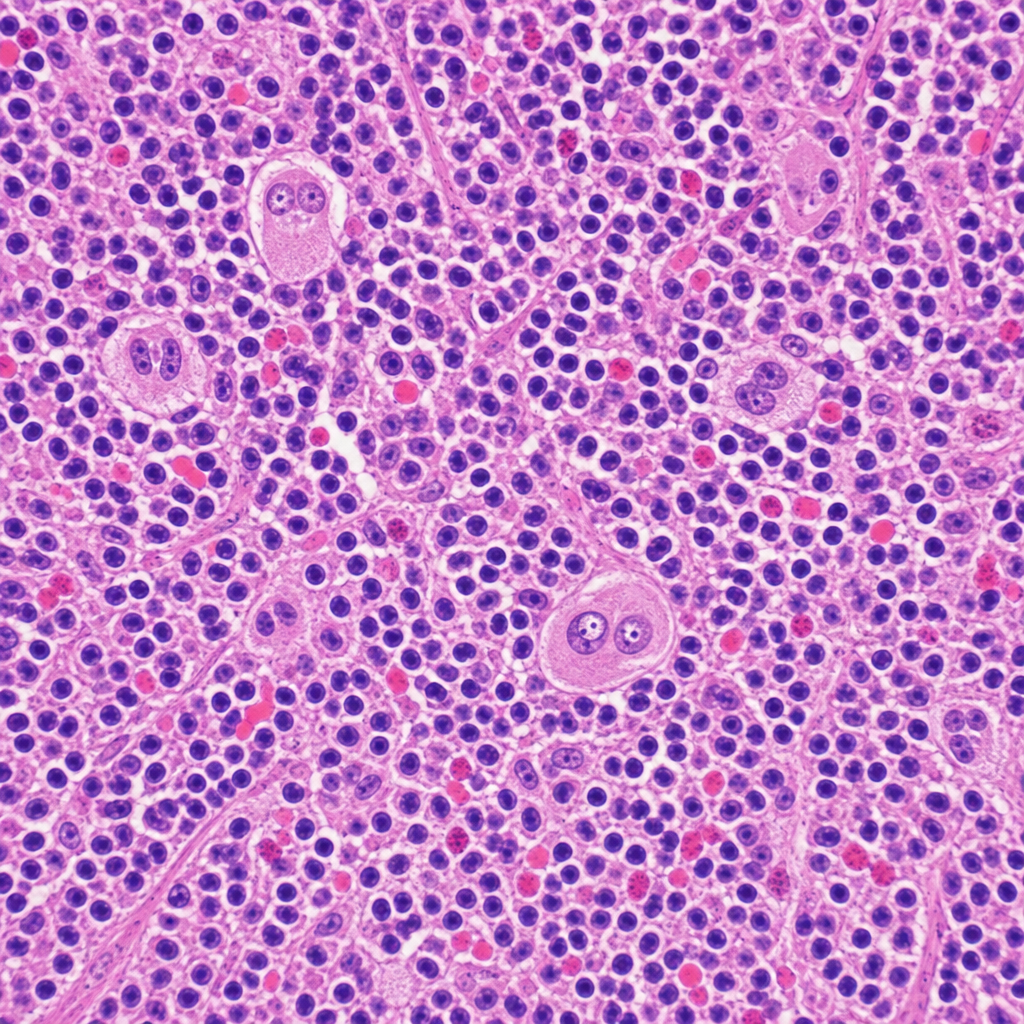
A 34-year-old woman presents with fatigue, night sweats, and a painless cervical lymph node mass for 3 months. Excisional biopsy of the lymph node is performed. The photomicrograph demonstrates a mixed cellular infiltrate with scattered large binucleated cells possessing prominent eosinophilic 'owl-eye' nucleoli, set against a background of lymphocytes, plasma cells, eosinophils, and fibroblasts. Immunohistochemical staining of the large cells is positive for CD15 and CD30 and negative for CD45. Which of the following best describes the cell of origin of the large binucleated cells seen in this lesion?
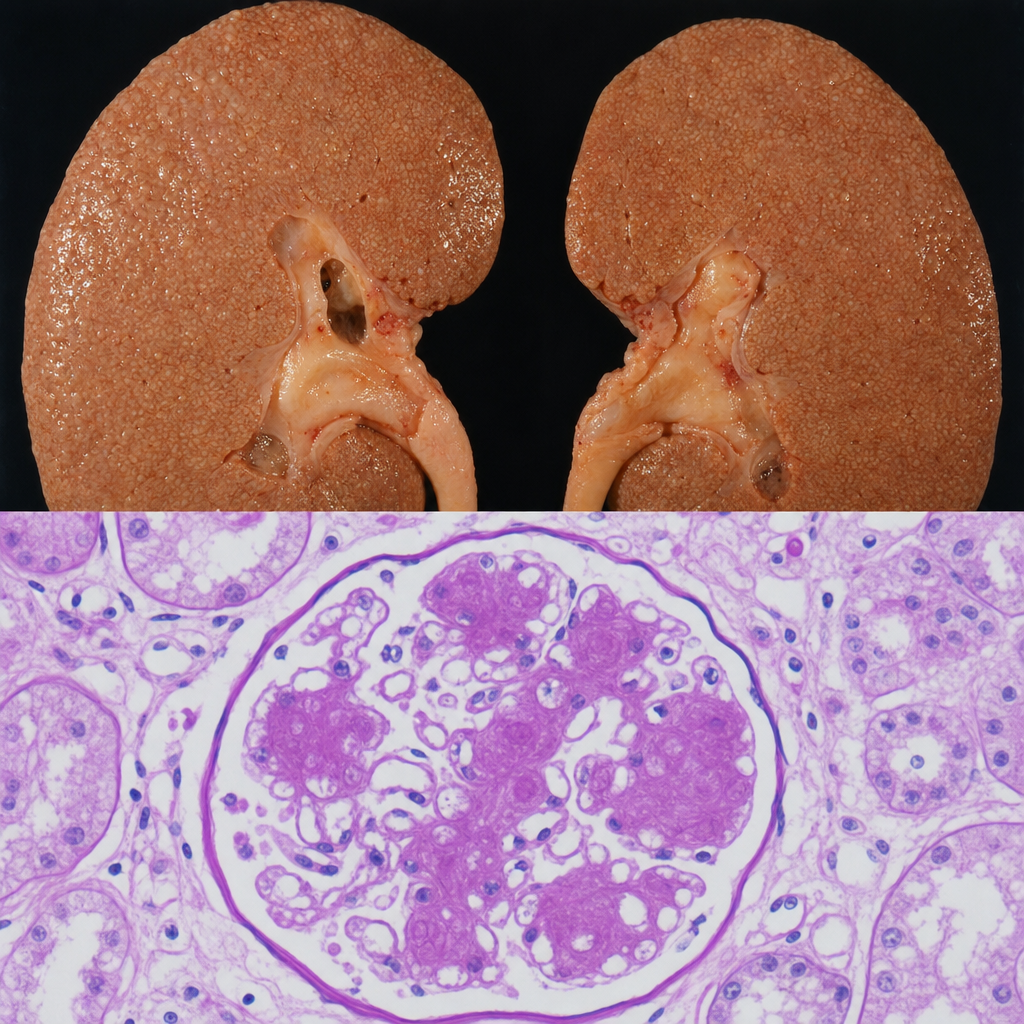
A 67-year-old man with a 20-year history of poorly controlled type 2 diabetes mellitus dies of a myocardial infarction. At autopsy, the kidneys are symmetrically enlarged with a granular cortical surface. PAS staining of the renal cortex shows PAS-positive ovoid deposits within the mesangium of glomeruli, compressing the adjacent capillary loops. Which of the following best describes the composition and pathogenetic mechanism of these deposits?
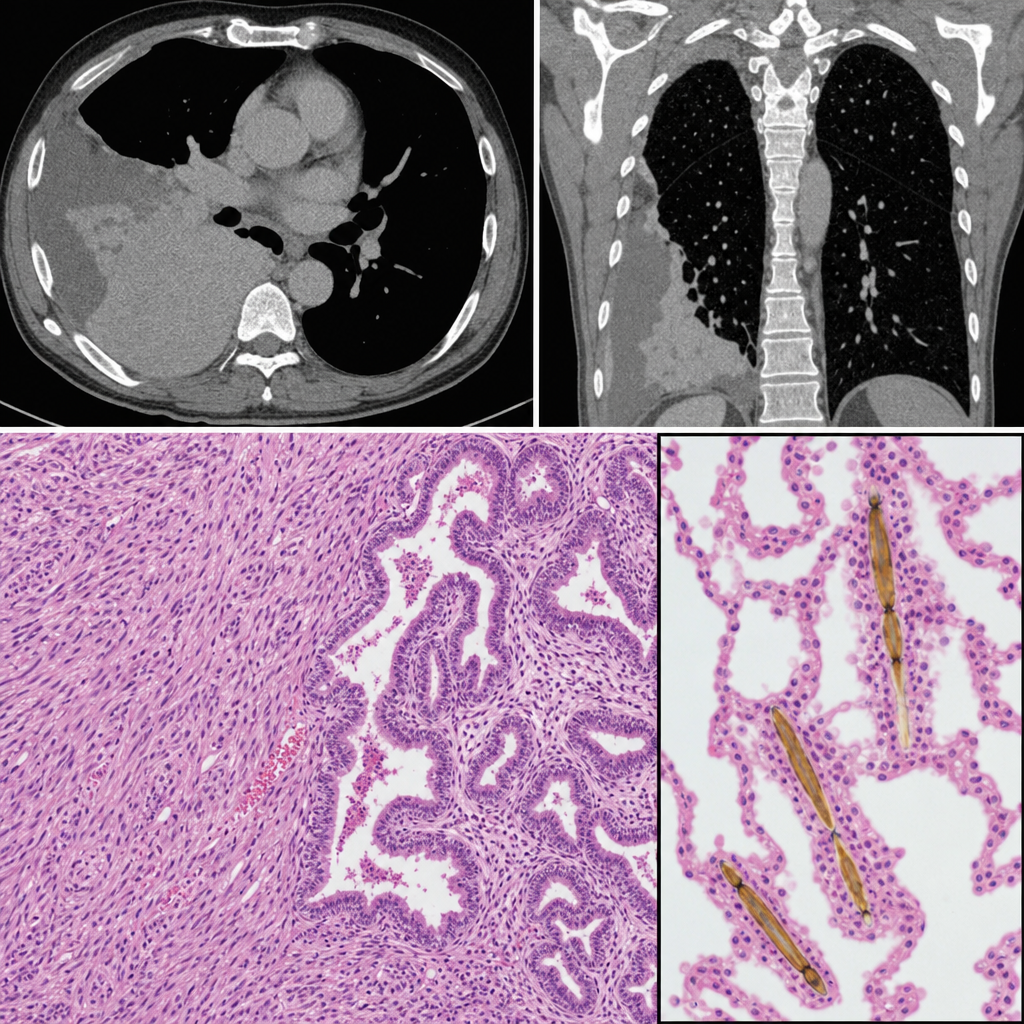
A 58-year-old man with a 40-pack-year smoking history presents with progressive dyspnea and a dry cough. Chest CT reveals bilateral pleural thickening and a right pleural mass. Thoracoscopic biopsy is performed. The photomicrograph shows a biphasic tumor with epithelioid cells forming tubulopapillary structures intermixed with a spindle-cell sarcomatoid component. Elongated, golden-brown, beaded structures with a translucent core are identified within the adjacent lung parenchyma, each coated with iron-protein complexes. Which of the following structures are most specifically represented by the coated inclusions seen in this specimen?
A 50-year-old woman with rheumatoid arthritis on methotrexate develops rapidly progressive painful ulcers on her legs with violaceous undermined borders. Biopsy shows neutrophilic dermal infiltrate with areas of necrosis, but no vasculitis or infection. Wound cultures are negative. Despite debridement, the ulcers worsen. C-ANCA and P-ANCA are negative. Evaluate the diagnosis and determine the management that addresses both the cutaneous condition and systemic disease.
A 25-year-old woman presents with painful oral ulcers and a pustular rash at venipuncture sites. She has genital ulcers and a history of recurrent uveitis. Skin biopsy from a pustule shows neutrophilic infiltrate in the dermis without vasculitis or infection. HLA-B51 testing is positive. She is planning pregnancy. Evaluate the management strategy considering disease control and pregnancy planning.
A 70-year-old man on chronic warfarin therapy presents with sudden onset of painful purpura on his thighs and buttocks three days after starting warfarin for atrial fibrillation. He has a history of multiple DVTs. Skin biopsy shows thrombosis of dermal blood vessels with minimal inflammation. Laboratory studies show an INR of 3.5. Evaluate the pathophysiology and determine the most appropriate immediate management.
A 35-year-old man presents with targetoid lesions on his palms and oral mucosa following treatment for Mycoplasma pneumonia. Skin biopsy shows necrotic keratinocytes throughout all layers of the epidermis with minimal inflammatory infiltrate. Direct immunofluorescence is negative. The patient develops similar lesions with each infection. Analyze the pathophysiology to identify the primary mechanism.
A 40-year-old woman with systemic lupus erythematosus presents with photosensitive facial erythema. Skin biopsy shows vacuolar interface dermatitis with thickened basement membrane, dermal mucin deposition, and perivascular lymphocytic infiltrate. Direct immunofluorescence shows granular deposits of IgG, IgM, and C3 at the dermal-epidermal junction. Analyze these findings to determine which additional laboratory test would best correlate with disease activity.
A 62-year-old woman presents with a pigmented lesion on her back. Biopsy shows atypical melanocytes arranged in nests at the dermal-epidermal junction and scattered as single cells through the epidermis with pagetoid spread. The melanocytes extend into the papillary dermis to a depth of 1.8 mm. No ulceration is present, and the mitotic rate is 3/mm². Analyze this pathology to determine the appropriate staging workup.
A 3-year-old boy presents with tense bullae on his trunk and extremities following a viral upper respiratory infection. Direct immunofluorescence shows linear IgA deposits along the basement membrane zone. Indirect immunofluorescence is negative. Apply this immunopathological pattern to select the most appropriate initial treatment.
Practice by Chapter
Inflammatory dermatoses
Practice Questions
Vesiculobullous diseases
Practice Questions
Infectious skin diseases
Practice Questions
Benign epithelial tumors
Practice Questions
Premalignant skin lesions
Practice Questions
Non-melanoma skin cancers
Practice Questions
Melanocytic nevi
Practice Questions
Melanoma pathology
Practice Questions
Adnexal tumors
Practice Questions
Dermal tumors and proliferations
Practice Questions
Panniculitis
Practice Questions
Vascular disorders of skin
Practice Questions
Disorders of pigmentation
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app