
Cell injury — MCQs

On this page
A 40-year-old man is rushed to the emergency department after being involved in a motor vehicle accident. He has lacerations on his right arm and some minor abrasions on his face and lower limbs. The resident on call quickly manages the patient with proper care of his open wounds in the emergency department. The patient is admitted to the surgery unit for the daily care of his wounds. His lacerations begin to heal with proper dressing and occasional debridement. Which of the following best describes the healing process in this patient?
A 7-year-old boy with a history of fetal alcohol syndrome is brought by his mother to the emergency room for malaise and lethargy. His mother reports that the family was on vacation in a cabin in the mountains for the past 10 days. Five days ago, the child developed a fever with a max temperature of 102.6°F (39.2°C). She also reports that he was given multiple medications to try to bring down his fever. Although his fever resolved two days ago, the child has become increasingly lethargic. He started having non-bilious, non-bloody emesis one day prior to presentation. His current temperature is 100°F (37.8°C), blood pressure is 95/55 mmHg, pulse is 110/min, and respirations are 22/min. On exam, the child is lethargic and minimally reactive. Mild hepatomegaly is noted. A biopsy of this patient's liver would likely reveal which of the following?
An investigator is studying intracellular processes in muscle tissue after denervation. A biopsy specimen is obtained from the biceps femoris muscle of an 82-year-old woman who sustained sciatic nerve injury. Investigation of the tissue specimen shows shrunken cells with dense eosinophilic cytoplasm, nuclear shrinkage, and plasma membrane blebbing. Which of the following best explains the muscle biopsy findings?
During an experiment, an investigator attempts to determine the rates of apoptosis in various tissue samples. Injecting cytotoxic T cells into the cell culture of one of the samples causes the tissue cells to undergo apoptosis. Apoptosis is most likely due to secretion of which of the following substances in this case?
A 21-year-old medical student is studying different types of necrosis and tissue injuries. In the pathology laboratory, he observes different dead tissues under the microscope and notices the changes that are occurring as a function of time. After serial observations, he deduced that coagulation necrosis is...?
A 40-year-old man presents with a rash, oral lesions, and vision problems for 5 days. He says the rash started as a burning feeling on his face and the upper part of his torso, but soon red spots appeared in that same distribution. The spots grew in size and spread to his upper extremities. The patient says the spots are painful but denies any associated pruritus. He says the painful oral lesions appeared about the same time as the rash. For the past 3 days, he also says he has been having double vision and dry, itchy eyes. He reports that he had a mild upper respiratory infection for a few days that preceded his current symptoms. The patient denies any chills, hematuria, abdominal or chest pain, or similar symptoms in the past. Past medical history is significant for a severe urinary tract infection diagnosed 3 weeks ago for which he has been taking trimethoprim-sulfamethoxazole. The vital signs include: temperature 38.3℃ (101.0℉), blood pressure 110/60 mm Hg, respiratory rate 20/min, and pulse 108/min. On physical examination, the patient has severe painful erosions of the oral mucosa. There are multiple fluid-filled vesicles and bullae averaging 3 mm in diameter with a surrounding erythematous ring that involve only the upper torso and extensor surfaces of upper extremities. Several of the lesions have ruptured, resulting in sloughing off of the epidermal layer. There is a prominent conjunctival injection present. Ophthalmic examination reveals mild bilateral corneal abrasions without any evidence of frank ulceration. Laboratory findings are significant for the following: White blood cell (WBC) count 8,500/mm3 Red blood cell (RBC) count 4.20 x 106/mm3 Hematocrit 41.5% Hemoglobin 14.0 g/dL Platelet count 215,000/mm3 C-reactive protein (CRP) 86 mg/L Urine and blood cultures are pending. Which of the following would confirm the most likely diagnosis in this patient?
A 50-year-old man arrives to the clinic complaining of progressive weakness. He explains that for 3 months he has had difficulty climbing the stairs, which has now progressed to difficulty getting out of a chair. He denies diplopia, dysphagia, dyspnea, muscle aches, or joint pains. He denies weight loss, weight gain, change in appetite, or heat or cold intolerance. He reports intermittent low-grade fevers. He has a medical history significant for hypertension and hyperlipidemia. He has taken simvastatin and losartan daily for the past 6 years. His temperature is 99.0°F (37.2°C), blood pressure is 135/82 mmHg, and pulse is 76/min. Cardiopulmonary examination is normal. The abdomen is soft, non-tender, non-distended, and without hepatosplenomegaly. Muscle strength is 3/5 in the hip flexors and 4/5 in the deltoids, biceps, triceps, patellar, and Achilles tendon reflexes are 2+ and symmetric. Sensation to pain, light touch, and vibration are intact. Gait is cautious, but grossly normal. There is mild muscle tenderness of his thighs and upper extremities. There is no joint swelling or erythema and no skin rashes. A complete metabolic panel is within normal limits. Additional lab work is obtained as shown below: Serum: Na+: 141 mEq/L Cl-: 100 mEq/L K+: 4.3 mEq/L HCO3-: 23 mEq/L Urea nitrogen: 18 mg/dL Glucose: 128 mg/dL Creatinine: 1.0 mg/dL Alkaline phosphatase: 69 U/L Aspartate aminotransferase (AST): 302 U/L Alanine aminotransferase (ALT): 210 U/L TSH: 6.9 uU/mL Thyroxine (T4): 5.8 ug/dL Creatine kinase: 4300 U/L C-reactive protein: 11.9 mg/L Erythrocyte sedimentation rate: 37 mm/h Which of the following is the most accurate diagnostic test?
An investigator is studying cellular repair mechanisms in various tissues. One of the samples being reviewed is from the anterior horn of the spinal cord of a patient who was involved in a snowboard accident. Pathologic examination of the biopsy specimen shows dispersion of the Nissl bodies, swelling of the neuronal body, and a displacement of the nucleus to the periphery in numerous cells. Which of the following is the most likely explanation for the observed findings?
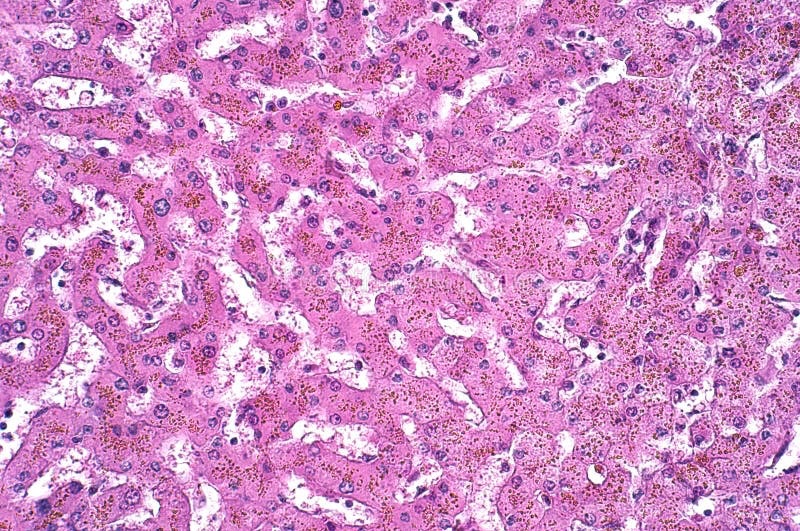
A previously healthy 44-year-old man comes to his physician because of frequent urination and increased thirst for several weeks. Physical examination shows darkened skin and a firm mass in the right upper quadrant. His blood glucose is 220 mg/dL. A photomicrograph of a specimen obtained on liver biopsy is shown. Which of the following best describes the pathogenesis of the disease process in this patient?
A 3-year-old boy is brought to the emergency department for nausea and vomiting for 1 day. His maternal uncle had a seizure disorder and died in childhood. He appears fatigued. Respirations are 32/min. Examination shows diffuse weakness in the extremities. Serum studies show a low pH, elevated lactate concentration, and normal blood glucose. A metabolic condition characterized by a defect in oxidative phosphorylation is suspected. Microscopic examination of a muscle biopsy specimen of this patient is most likely to show which of the following findings?
Practice by Chapter
Reversible cell injury mechanisms
Practice Questions
Irreversible cell injury (necrosis)
Practice Questions
Types of necrosis (coagulative, liquefactive, etc.)
Practice Questions
Apoptosis pathways
Practice Questions
Autophagy mechanisms
Practice Questions
Cellular adaptations (atrophy, hypertrophy)
Practice Questions
Hyperplasia and metaplasia
Practice Questions
Dysplasia
Practice Questions
Intracellular accumulations
Practice Questions
Pathologic calcification
Practice Questions
Cellular aging mechanisms
Practice Questions
Ischemia-reperfusion injury
Practice Questions
Free radical injury
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app