
Cell injury — MCQs

On this page
A 37-year-old man presents to the clinic because of painful, severe blistering over his buttocks for the past week. About a year ago, he noticed a similar outbreak on his inner thighs, but it receded within a few days on its own. Physical examination shows the blisters are tense, and rubbing the affected skin does not result in ‘popping’ of the blisters. A biopsy shows the entire epidermis lifting away from the basal lamina with extensive inflammatory infiltrates abundant with eosinophils. Immunofluorescence shows a linear pattern of immune complex deposits. Which of the following cellular structures, if defective, is most likely involved in the formation of these blisters?
A 48-year-old man has smoked approximately 3 packs of cigarettes per day for the past 12 years. Which of the following pathologic changes is most likely to occur in his bronchial epithelium?
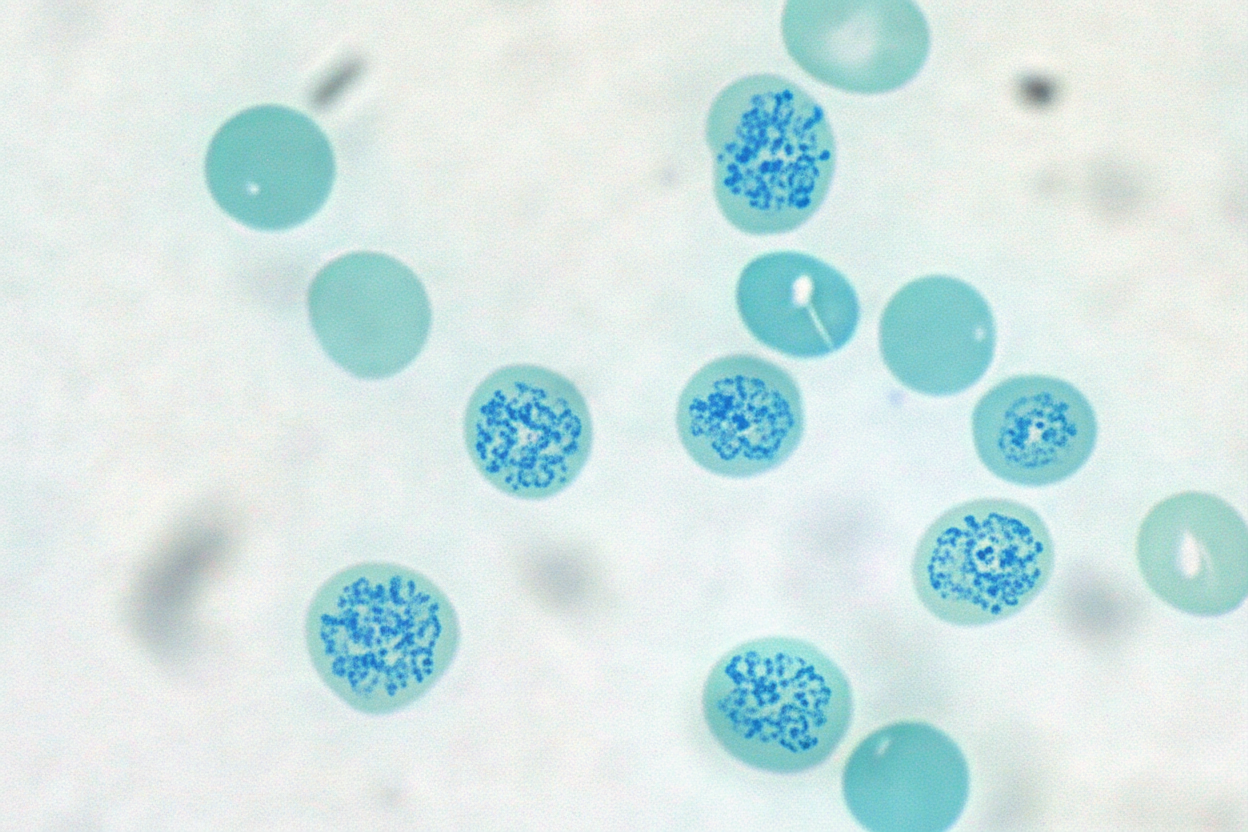
A 59-year-old woman with a history of chronic kidney disease comes to the physician for a 3-month history of easy fatiguability. Physical examination shows subconjunctival pallor. Her hemoglobin concentration is 8.9 g/dL, mean corpuscular volume is 86 μm3, and serum ferritin is 225 ng/mL. Treatment with erythropoietin is begun. A peripheral blood smear is obtained one week after treatment. A photomicrograph of the smear after specialized staining is shown. The prominent color of the intracellular structure in some of the cells is most likely the result of staining which of the following?
A 30-year-old woman presents to her physician for a routine check-up. She says she is planning to get pregnant. Past medical history is significant for arterial hypertension. Current medications are enalapril. The physician explains that this medication can be teratogenic. He changes her antihypertensive medication to methyldopa, which has no contraindications for pregnant women. A few days later, the patient is admitted to the emergency department with jaundice and dark urine. Her laboratory tests are as follows: Hemoglobin 0.9 g/dL Red blood cells 3.2 x 106/µL White blood cells 5,000/mm3 Platelets 180,000/mm3 Direct Coombs test Positive This patient is diagnosed with autoimmune hemolytic anemia (AIHA). Which of the following is correct about autoimmune hemolytic anemia in this patient?
A previously healthy 5-year-old girl is brought to the emergency department by her parents because of a severe headache, nausea, and vomiting for 6 hours. Last week she had fever, myalgias, and a sore throat for several days that resolved with over-the-counter medication. She is oriented only to person. Examination shows bilateral optic disc swelling. Serum studies show: Glucose 61 mg/dL Aspartate aminotransferase (AST) 198 U/L Alanine aminotransferase (ALT) 166 U/L Prothrombin time 18 sec Which of the following is the most likely cause of this patient's symptoms?
An autopsy is being performed on an elderly man who died from a myocardial infarction. Biopsy of the heart is likely to reveal necrosis most similar to necrosis seen in which of the following scenarios?
A 30-year-old man comes to the physician for a follow-up examination 1 month after sustaining a chemical burn over the dorsum of his right hand and forearm. Physical examination shows hyperextension of the hand at the wrist. The skin over the dorsum of the wrist is tense and there is a thick, epithelialized scar. Range of motion of the right wrist is restricted. This patient's contracture is most likely due to activity of which of the following cells?
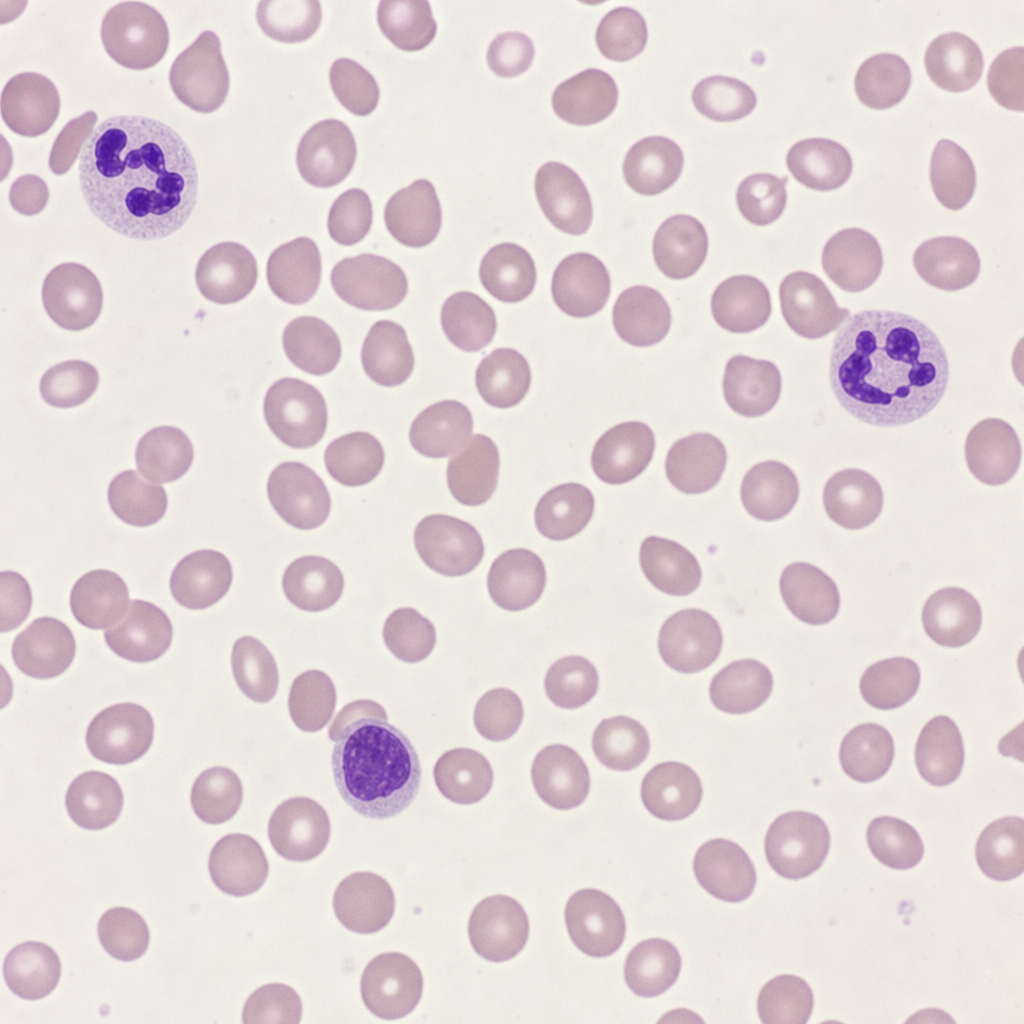
A 59-year-old man presents with fatigue and tingling in both feet and hands. Past medical history is significant for type 2 diabetes mellitus diagnosed 27 years ago, for which he takes metformin and gliclazide. He denies any smoking, alcohol, or illicit drug use. Physical examination is unremarkable. Laboratory results reveal the following: Hemoglobin 10.4 g/dL Hematocrit 31% Mean corpuscular volume 110 μm3 Corrected reticulocyte index low Leukocyte count 7,500 /mm3 Platelet count 250,000 /mm3 A peripheral blood smear is shown in the exhibit (see image). Which of the following best describes the underlying cause of this patient’s anemia?
An 8-year-old boy presents with a 7-day history of fever and abdominal pain for the past 4 days. Past medical history is significant for an exchange transfusion for neonatal hyperbilirubinemia and recurrent attacks of pallor during the course of upper respiratory tract infections. His vital signs include: blood pressure 120/70 mm Hg, pulse 105/min, respiratory rate 40/min, and temperature 37.0℃ (98.6℉). On physical examination, the patient is ill-looking. Conjunctivae are pale and the sclera is icteric. The liver is palpable 2 cm below the costal margin and the spleen is palpable 3 cm below the left costal margin. Laboratory findings show hemoglobin of 5.9 gm/dL, Hct of 20%, and haptoglobin of 28 mg/dL. A peripheral blood smear shows hypochromic anemia, polychromasia, anisocytosis, and occasional Heinz bodies. The reticulocyte count was 15%. A direct Coombs test was negative. Which of the following is the most likely diagnosis in this patient?
A 3-year-old boy is brought to the physician because of a 1-week history of yellowish discoloration of his eyes and skin. He has had generalized fatigue and mild shortness of breath for the past month. Three weeks ago, he was treated for a urinary tract infection with antibiotics. His father underwent a splenectomy during childhood. Examination shows pale conjunctivae and jaundice. The abdomen is soft and nontender; there is nontender splenomegaly. Laboratory studies show: Hemoglobin 9.1 g/dL Mean corpuscular volume 89 μm3 Mean corpuscular hemoglobin 32 pg/cell Mean corpuscular hemoglobin concentration 37.8% Hb/cell Leukocyte count 7800/mm3 Platelet count 245,000/mm3 Red cell distribution width 22.8% (N=13%–15%) Serum Bilirubin Total 13.8 mg/dL Direct 1.9 mg/dL Lactate dehydrogenase 450 U/L Which of the following is the most likely pathophysiology of these findings?
Practice by Chapter
Reversible cell injury mechanisms
Practice Questions
Irreversible cell injury (necrosis)
Practice Questions
Types of necrosis (coagulative, liquefactive, etc.)
Practice Questions
Apoptosis pathways
Practice Questions
Autophagy mechanisms
Practice Questions
Cellular adaptations (atrophy, hypertrophy)
Practice Questions
Hyperplasia and metaplasia
Practice Questions
Dysplasia
Practice Questions
Intracellular accumulations
Practice Questions
Pathologic calcification
Practice Questions
Cellular aging mechanisms
Practice Questions
Ischemia-reperfusion injury
Practice Questions
Free radical injury
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app