
Cell injury — MCQs

On this page
A 3-year-old boy is brought to the physician for a well-child examination. He has had multiple falls while walking and running for the past 4 months. He used to be able to climb stairs independently but now requires assistance. He started speaking in 2-word sentences at 2 years of age. He is at the 50th percentile for height and the 60th percentile for weight. Examination shows a waddling gait and enlargement of bilateral calves. Muscle strength is decreased in the bilateral lower extremities. Patellar and ankle reflexes are 1+ bilaterally. To rise from a sitting position, he uses his hands to support himself to an upright position. Diagnosis is confirmed by a muscle biopsy and immunohistochemistry. Which of the following is most likely responsible for the most severe clinical presentation of this disease?
A 72-year-old female is brought to the emergency department by ambulance because she was unable to walk. She says that she cut her leg while falling about a week ago. Since then, the wound has started draining fluid and become progressively more painful. She is found to have necrotizing fasciitis and is taken emergently to the operating room. Histological examination of cells along the fascial planes reveal cells undergoing necrosis. Which of the following represents the earliest sign that a cell has progressed to irreversible damage in this patient?
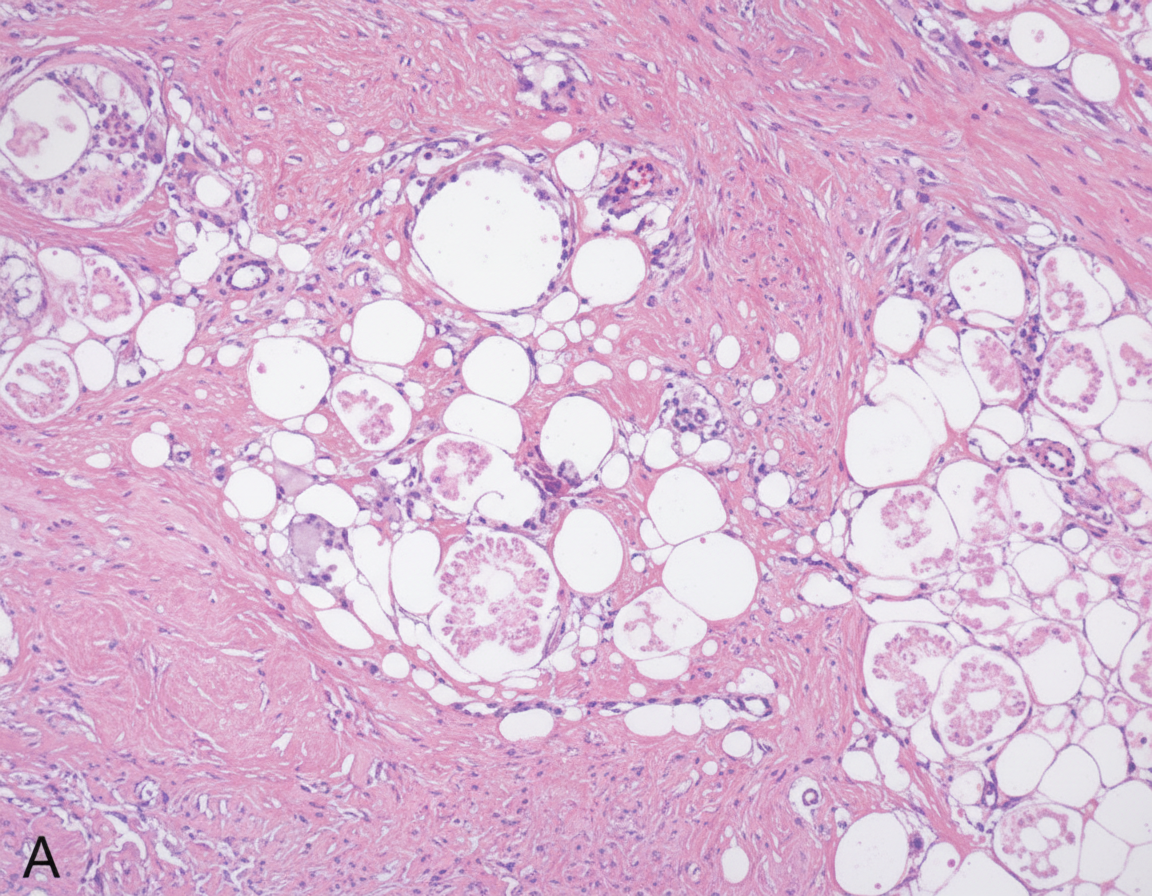
A 34-year-old woman comes to the physician a week after noticing a lump in her left breast. Three months ago, she was discharged from the hospital after treatment of multiple injuries sustained in a motor vehicle collision. Her only medication is an oral contraceptive. Her mother died of ovarian cancer. Examination shows a 2.5-cm, nontender mass in the upper outer quadrant of the left breast. Mammography shows a circumscribed radiolucent lesion with a rim of peripheral calcification. A photomicrograph of tissue from a biopsy of the mass is shown. Which of the following is the most likely cause of the breast swelling?
An 8-month-old boy presents with poor feeding. The patient’s mother says that he has refused to eat since yesterday morning. She also noticed that he has had trouble keeping his head up and appears floppy. She had breastfed him exclusively and just recently introduced him to pureed foods. His last bowel movement was 3 days ago which was normal. Past medical history is significant for recent otitis media. No current medications except for herbal supplements administered by his parents. Patient is not immunized due to the parent’s religious beliefs. The vital signs include: temperature 37.0°C (98.6°F), blood pressure 85/45 mm Hg, pulse 140/min, respiratory rate 31/min, and oxygen saturation 99% on room air. On physical examination, the patient is lethargic and drooling. Flaccid muscle tone present in all extremities. There is bilateral ptosis with sluggish pupillary reflexes. Which of the following best describes the pathophysiology of this patient’s condition?
A 56-year-old woman presents to the clinic complaining of fatigue and nausea. She was recently diagnosed with metastatic ovarian cancer and subsequently started treatment with an alkylating agent. The patient reports recent weight loss, malaise, and drowsiness, but denies fever, headaches, palpitations, shortness of breath, or genitourinary symptoms. Physical exam was unremarkable. Laboratory tests are shown below. Serum: Na+: 137 mEq/L Cl-: 101 mEq/L K+: 4.8 mEq/L HCO3-: 25 mEq/L BUN: 8.5 mg/dL Glucose: 117 mg/dL Creatinine: 2.1 mg/dL Thyroid-stimulating hormone: 1.8 µU/mL Ca2+: 9.6 mg/dL AST: 8 U/L ALT: 11 U/L What findings on urinalysis are most specific to this patient’s diagnosis?
A biology student is studying apoptosis pathways. One of the experiments conducted involves the binding of a ligand to a CD95 receptor. A defect of this pathway will most likely cause which of the conditions listed below?
A 68-year-old man is brought to the physician by his wife because she is concerned about his speech being irregular. Specifically, she says that over the last 8 months, her husband has been saying increasingly nonsensical statements at home. In addition, he is no longer able to perform basic verbal tasks such as ordering from a menu or giving directions even though he was an English teacher prior to retirement. She also reports that he has recently started attempting to kiss strangers and urinate in public. Finally, she has also noticed that he has been frequently binge eating sweets even though he was previously very conscientious about his health. When asked about these activities, the patient does not have insight into his symptoms. Which of the following would most likely be seen in this patient?
A 29-year-old woman presents with a 2-hour history of sudden onset of severe mid-epigastric pain. The pain radiates to the back, and is not relieved by over-the-counter antacids. The patient also complains of profuse vomiting. The patient’s medical history is negative for similar symptoms. She consumes 3–4 alcoholic drinks daily. The blood pressure is 80/40 mm Hg and the heart rate is 105/min. Examination of the lungs reveals bibasilar crackles. Abdominal examination reveals diffuse tenderness involving the entire abdomen, marked guarding, rigidity, and reduced bowel sounds. The chest X-ray is normal. However, the abdominal CT scan reveals peritoneal fluid collection and diffuse pancreatic enlargement. The laboratory findings include: Aspartate aminotransferase 63 IU/L Alkaline phosphatase 204 IU/L Alanine aminotransferase 32 IU/L Serum amylase 500 IU/L (Normal: 25-125 IU/L) Serum lipase 1,140 IU/L (Normal: 0-160 IU/L) Serum calcium 2 mmol/L Which of the following cellular changes are most likely, based on the clinical and laboratory findings?
A 65-year-old man presents with generalized edema and dyspnea on exertion. He also complains of easy bruising and nasal bleeding. Past medical history is significant for a right-sided myocardial infarction 4 years ago. Current medications are metoprolol, aspirin, and rosuvastatin. His vital signs are as follows: blood pressure 140/90 mm Hg, heart rate 78/min, respiratory rate 17/min, and temperature 36.5℃ (97.7℉). On physical examination, the patient is pale and acrocyanotic with cold extremities. Cardiac examination shows the right displacement of the apical beat, decreased heart sounds, and the presence of an S3. Abdominal percussion reveals ascites and hepatomegaly. Which of the following hepatic cell types is most sensitive to ischemia?
An 84-year-old man is brought to the physician by the staff of a group home where he resides because of worsening confusion and decreased urinary output. His nurse reports that the patient has not been drinking much for the last 3 days. Examination shows a decreased skin turgor and dry oral mucosa. His pulse is 105/min and blood pressure is 100/65 mm Hg. His serum creatinine is 3.1 mg/dL and a urea nitrogen is 42 mg/dL. Urine studies show multiple brownish granular casts. Which of the following processes is most likely involved in the pathogenesis of this patient's condition?
Practice by Chapter
Reversible cell injury mechanisms
Practice Questions
Irreversible cell injury (necrosis)
Practice Questions
Types of necrosis (coagulative, liquefactive, etc.)
Practice Questions
Apoptosis pathways
Practice Questions
Autophagy mechanisms
Practice Questions
Cellular adaptations (atrophy, hypertrophy)
Practice Questions
Hyperplasia and metaplasia
Practice Questions
Dysplasia
Practice Questions
Intracellular accumulations
Practice Questions
Pathologic calcification
Practice Questions
Cellular aging mechanisms
Practice Questions
Ischemia-reperfusion injury
Practice Questions
Free radical injury
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app