
Cell injury — MCQs

On this page
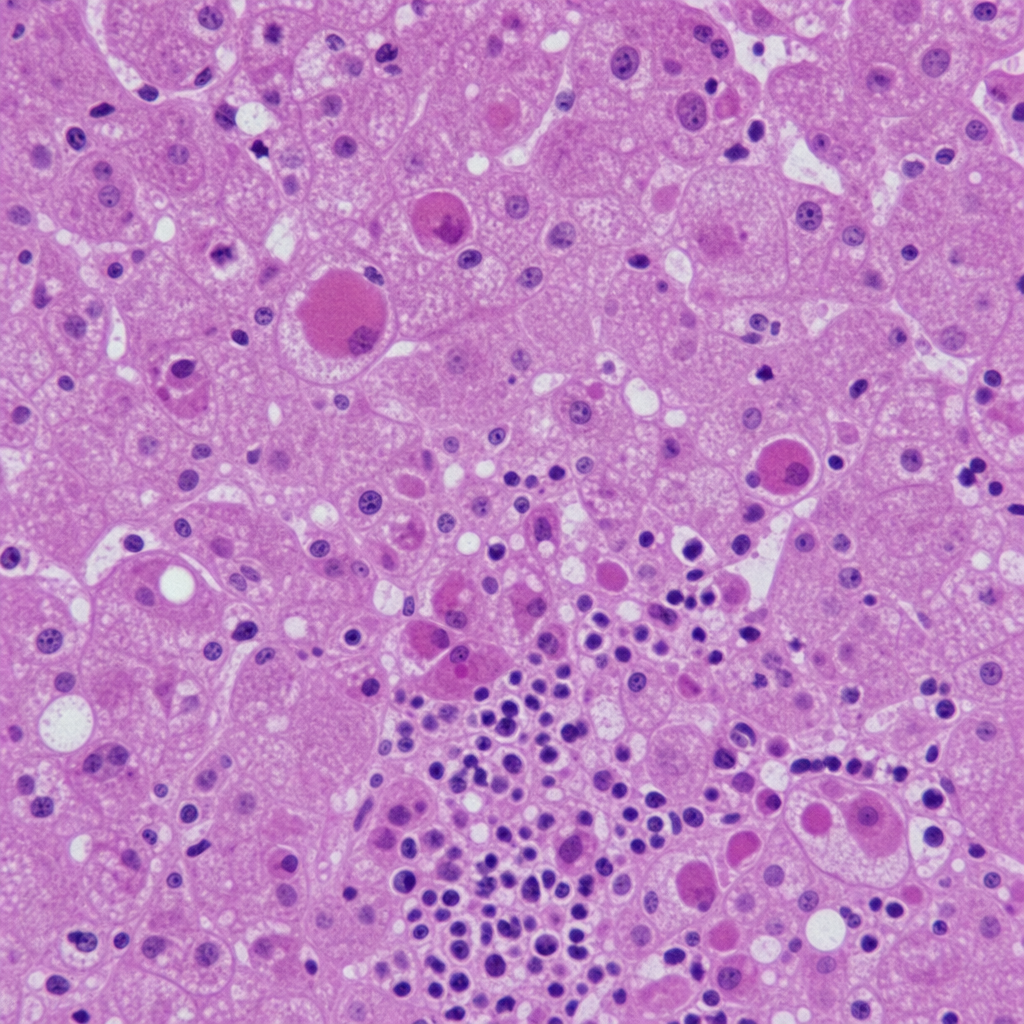
A 55-year-old man with a long history of alcohol use disorder presents with jaundice, tender hepatomegaly, and fever. A liver biopsy is performed. The biopsy demonstrates hepatocytes containing irregular rope-like eosinophilic cytoplasmic inclusions, ballooning degeneration of hepatocytes, neutrophilic infiltration predominantly in zone 3 (centrilobular region), and scattered acidophil bodies. Which of the following best identifies the cytoplasmic inclusions depicted and their composition?
Practice by Chapter
Reversible cell injury mechanisms
Practice Questions
Irreversible cell injury (necrosis)
Practice Questions
Types of necrosis (coagulative, liquefactive, etc.)
Practice Questions
Apoptosis pathways
Practice Questions
Autophagy mechanisms
Practice Questions
Cellular adaptations (atrophy, hypertrophy)
Practice Questions
Hyperplasia and metaplasia
Practice Questions
Dysplasia
Practice Questions
Intracellular accumulations
Practice Questions
Pathologic calcification
Practice Questions
Cellular aging mechanisms
Practice Questions
Ischemia-reperfusion injury
Practice Questions
Free radical injury
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app