
Cardiovascular — MCQs

On this page
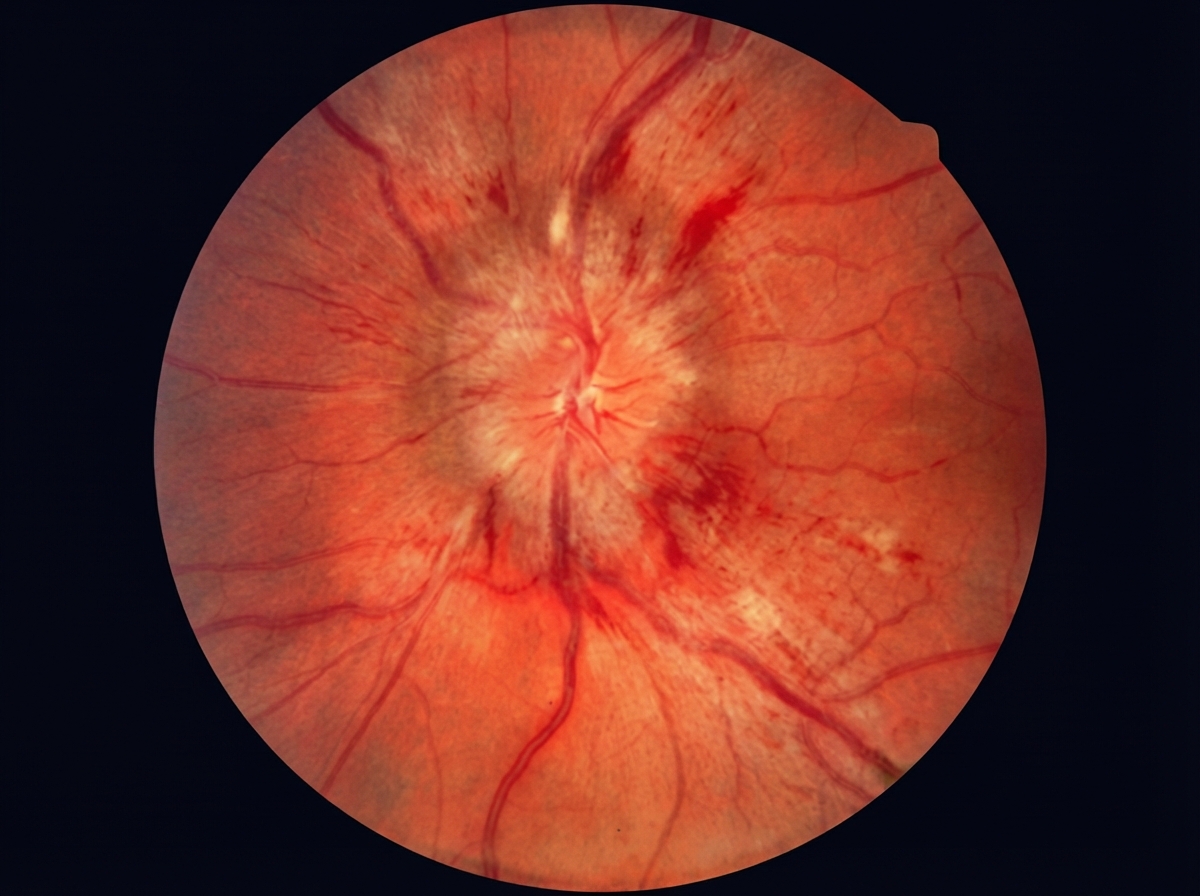
A 55-year-old man visits his primary care physician for a follow-up visit. He was diagnosed with asthma during childhood, but it has always been well controlled with an albuterol inhaler. He is hypertensive and admits that he is not compliant with his antihypertensive medication. He expresses his concerns about frequent headaches and blurry vision over the past few months. He has been taking acetaminophen for his headaches, but it has not made any difference. The blood pressure is 220/130 mm Hg, pulse rate is 77/min, and respiratory rate is 14/min. The BMI is 36.2 kg/m2. Physical examination is unremarkable. A urinalysis is notable for proteinuria. Funduscopic examination is shown on the right. Which finding best explains the changes seen in this patient's fundoscopic examination? (Note: the dominant finding is optic disc edema; retinal hemorrhages are also present but are not the primary finding being tested.)
A 65-year-old woman presents with severe abdominal pain and bloody diarrhea. Past medical history is significant for a myocardial infarction 6 months ago. The patient reports a 25-pack-year smoking history and consumes 80 ounces of alcohol per week. Physical examination shows a diffusely tender abdomen with the absence of bowel sounds. Plain abdominal radiography is negative for free air under the diaphragm. Laboratory findings show a serum amylase of 115 U/L, serum lipase 95 U/L. Her clinical condition deteriorates rapidly, and she dies. Which of the following would most likely be the finding on autopsy in this patient?
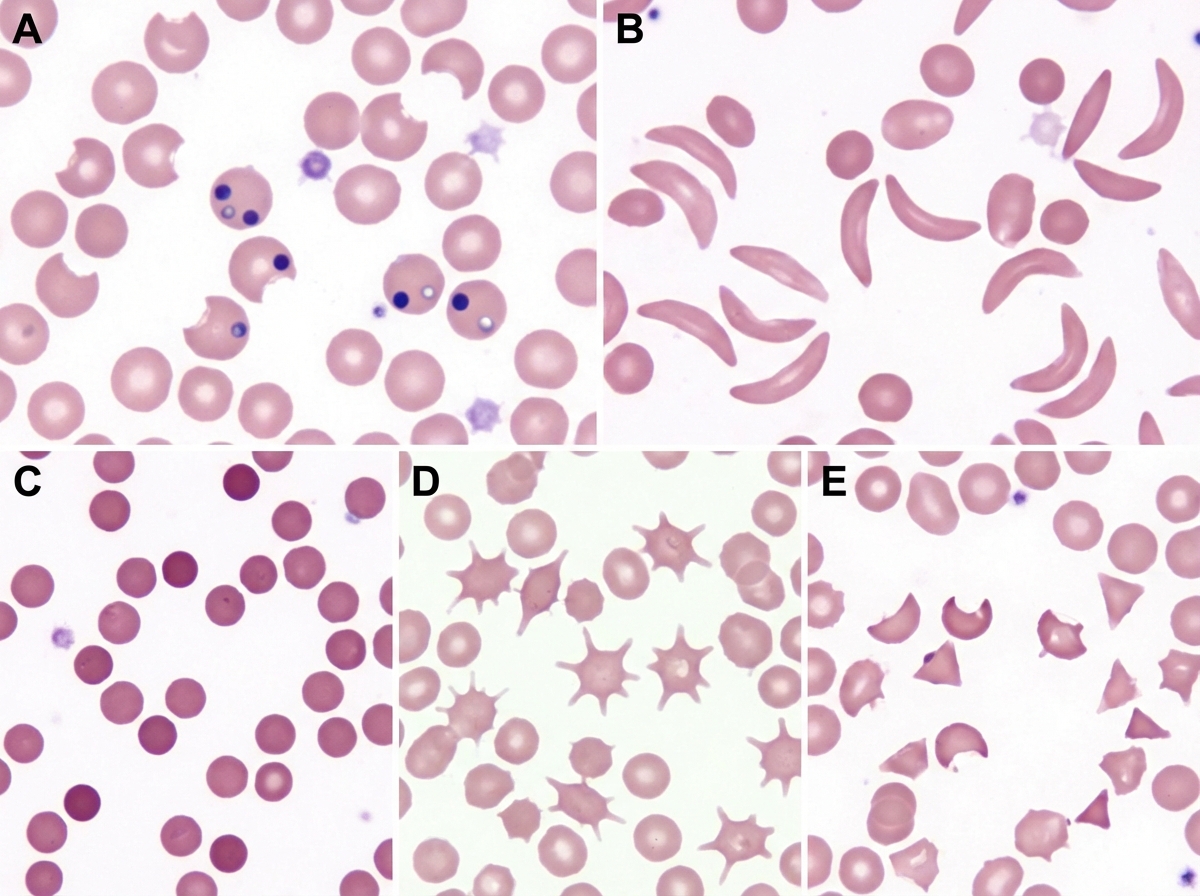
A 68-year-old man of Mediterranean descent comes to the clinic with complaints of fatigue for the past month. He reports that it is increasingly difficult for him to complete his after-dinner walks as he would get breathless and tired around 10 minutes. He endorses dizziness and an upper respiratory infection last week for which he "took a lot of aspirin." Past medical history is significant for malaria 10 years ago (for which he was adequately treated with anti-malarial medications) and aortic stenosis status post prosthetic valve replacement 5 months ago; a recent echocardiogram confirms normal prosthetic valve function with no paravalvular leak or evidence of mechanical hemolysis. When asked if he has had similar episodes before, he claims, "Never! I've been as healthy as a horse until my heart surgery." Laboratory results show elevated indirect bilirubin and LDH, low haptoglobin. Physical examination is significant for mild scleral icterus bilaterally and a faint systolic murmur. Which of the following images represents a potential peripheral smear in this patient?
A 31-year-old Israeli male with a history of heavy smoking presents to your office with painful ulcerations on his hands and feet. Upon examination, he is found to have hypersensitivity to intradermally injected tobacco extract. Which of the following processes is most likely responsible for his condition?
A 15-year-old African-American boy is brought to the physician because of left-sided groin pain and difficulty walking for 3 weeks. He reports having pain at rest and increased pain with activity. He recently started playing flag football but does not recall any trauma. He has had many episodes of joint and bone pain that required hospitalization in the past. He is at the 25th percentile for height and 20th percentile for weight. His temperature is 37°C (98.6°F), blood pressure is 120/80 mm Hg, and pulse is 90/min. Examination shows tenderness over the lateral aspect of the hip with no swelling, warmth, or erythema. There is pain with passive internal rotation of the left hip. The remainder of the examination shows no abnormalities. Leukocyte count is 9,000/mm3. Which of the following conditions is the most likely cause of the patient's current symptoms?
A previously healthy 82-year-old man dies in a motor vehicle collision. At autopsy, the heart shows slight ventricular thickening. There are abnormal, insoluble aggregations of protein filaments in beta-pleated linear sheets in the ventricular walls and, to a lesser degree, in the atria and lungs. No other organs show this abnormality. Bone marrow examination shows no plasma cell dyscrasia. The abnormal protein aggregations are most likely composed of which of the following?
A 56-year-old male died in a motor vehicle accident. Autopsy reveals extensive atherosclerosis of his left anterior descending artery marked by intimal smooth muscle and collagen proliferation. Which of the following is implicated in recruiting smooth muscle cells from the media to intima in atherosclerotic lesions?
A 54-year-old man was brought to the emergency room due to acute onset of slurred speech while at work, after which he lost consciousness. The patient's wife says this occurred approximately 30 minutes ago. Past medical history is significant for poorly controlled hypertension and type 2 diabetes mellitus. His blood pressure is 90/50 mm Hg, respiratory rate is 12/min, and heart rate is 48/min. The patient passes away shortly after arriving at the hospital. At autopsy, bilateral wedge-shaped strips of necrosis are seen in this patient's brain in the medial temporal lobe structures. Which of the following is the most likely location of these necrotic cells?
An 18-year-old man presents with a sudden loss of consciousness while playing college football. There was no history of a concussion. Echocardiography shows left ventricular hypertrophy and increased thickness of the interventricular septum. Which is the most likely pathology underlying the present condition?
A 72-year-old man who was involved in a traffic collision is brought to the emergency room by the ambulance service. He was in shock and comatose at the time of presentation. On examination, the heart rate is 60/min, and the blood pressure is 70/40 mm Hg. The patient dies, despite resuscitative efforts. Autopsy reveals multiple internal hemorrhages and other evidence of ischemic damage affecting the lungs, kidneys, and brain. The patient’s heart shows evidence of gross anomaly similar to the picture. While acute hypovolemia is the likely cause of the ischemic changes seen in the lungs, kidneys, and brain, which of the following best explains the gross anomaly of his heart?

Practice by Chapter
Atherosclerosis
Practice Questions
Ischemic heart disease
Practice Questions
Myocardial infarction pathology
Practice Questions
Hypertensive heart disease
Practice Questions
Congenital heart defects
Practice Questions
Valvular heart disease
Practice Questions
Rheumatic heart disease
Practice Questions
Infective endocarditis
Practice Questions
Myocarditis and cardiomyopathies
Practice Questions
Pericardial diseases
Practice Questions
Aneurysms and dissections
Practice Questions
Vasculitis
Practice Questions
Cardiac tumors
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app