
Myocarditis and cardiomyopathies — MCQs

A 43-year-old woman presents to her primary care provider with shortness of breath. She reports a 4-month history of progressively worsening difficulty breathing with associated occasional chest pain. She is a long-distance runner but has had trouble running recently due to her breathing difficulties. Her past medical history is notable for well-controlled hypertension for which she takes hydrochlorothiazide. She had a tibial osteosarcoma lesion with pulmonary metastases as a child and successfully underwent chemotherapy and surgical resection. She has a 10 pack-year smoking history but quit 15 years ago. She drinks a glass of wine 3 times per week. Her temperature is 98.6°F (37°C), blood pressure is 140/85 mmHg, pulse is 82/min, and respirations are 18/min. On exam, she has increased work of breathing with a normal S1 and loud P2. An echocardiogram in this patient would most likely reveal which of the following?
A 72-year-old African American man presents with progressive fatigue, difficulty breathing on exertion, and lower extremity swelling for 3 months. The patient was seen at the emergency department 2 times before. The first time was because of back pain, and the second was because of fever and cough. He took medications at the emergency room, but he refused to do further tests recommended to him. He does not smoke or drink alcohol. His family history is irrelevant. His vital signs include a blood pressure of 110/80 mm Hg, temperature of 37.2°C (98.9°F), and regular radial pulse of 90/min. On physical examination, the patient looks pale, and his tongue is enlarged. Jugular veins become distended on inspiration. Pitting ankle edema is present on both sides. Bilateral basal crackles are audible on the chest auscultation. Hepatomegaly is present on abdominal palpation. Chest X-ray shows osteolytic lesions of the ribs. ECG shows low voltage waves and echocardiogram shows a speckled appearance of the myocardium with diastolic dysfunction and normal appearance of the pericardium. Which of the following best describes the mechanism of this patient’s illness?
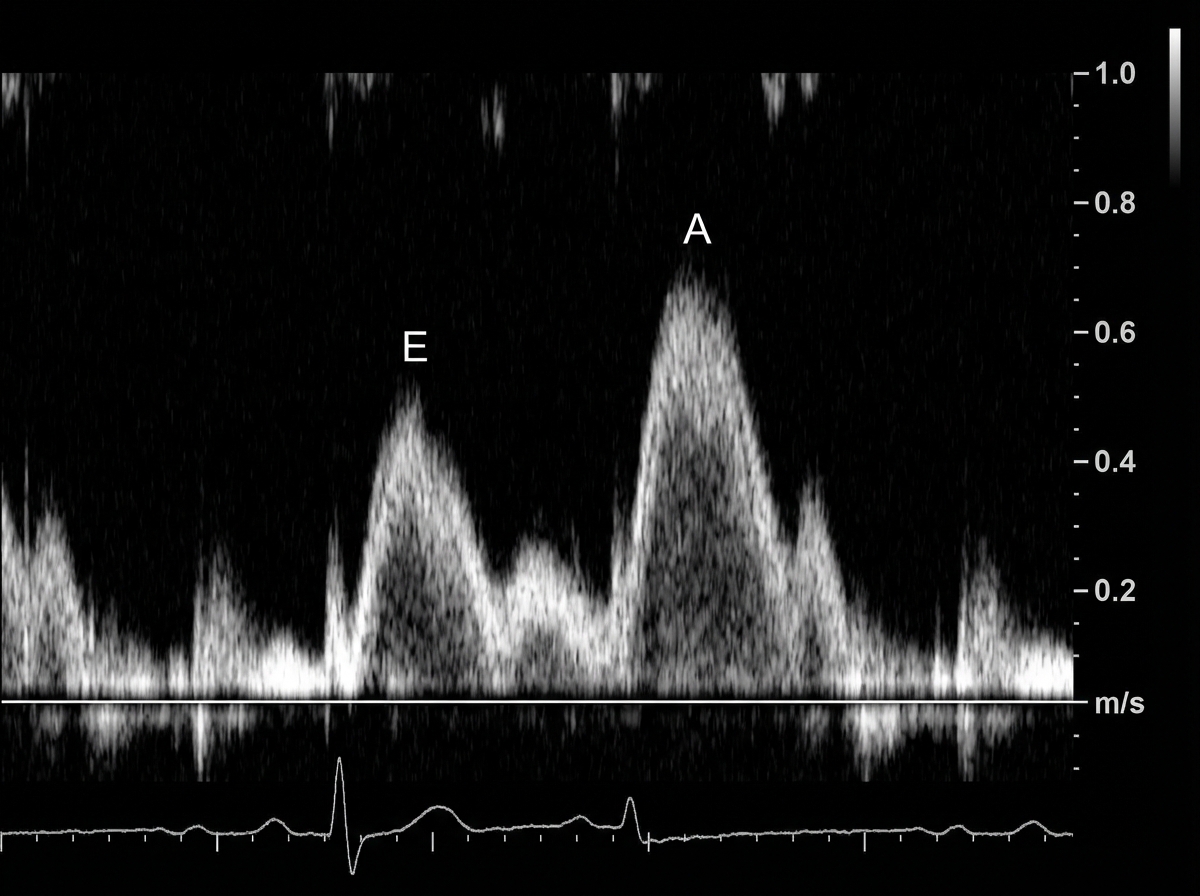
A 49-year-old man presents to his physician complaining of weakness and fatigue. On exam, you note significant peripheral edema. Transthoracic echocardiogram is performed and reveals a preserved ejection fraction with impaired diastolic relaxation. A representative still image is shown in Image A. Which of the following is likely the cause of this patient's symptoms?
A 22-year-old male varsity athlete visits the on-campus health services for shortness of breath, fatigue, and lower limb edema with onset 1 week after mild upper respiratory tract infection. Upon physical examination, his blood pressure is 100/68 mm Hg, heart rate is 120/min, respiratory rate is 23/min, and temperature is 36.4°C (97.5°F). He is referred to the nearest hospital, where his systolic pressure drops below 90 mm Hg with an S3 gallop, and he needs inotropic support in the critical care unit. A chest radiograph shows an enlarged heart, clear lungs, and effacement of the right costodiaphragmatic angle. A subsequent esophageal echocardiogram reveals severe dilation of all heart cavities, an ejection fraction of 23%, and mitral regurgitation. His family and personal history are unremarkable; therefore, an endomyocardial biopsy (EMB) is ordered. Which of the following microscopic findings would you expect in this specimen?
A 28-year-old man presents to the clinic with increasing shortness of breath, mild chest pain at rest, and fatigue. He normally lives a healthy lifestyle with moderate exercise and an active social life, but recently he has been too tired to do much. He reports that he is generally healthy and on no medications but did have a ‘cold’ 2 weeks ago. He does not smoke, besides occasional marijuana with friends, and only drinks socially. His father has hypertension, hyperlipidemia, and lung cancer after a lifetime of smoking, and his mother is healthy. He also has one older brother with mild hypertension. His pulse is 104/min, the respiratory rate 23/min, the blood pressure 105/78 mm Hg, and the temperature 37.1°C (98.8°F). On physical examination, he is ill-appearing and has difficulty completing sentences. On auscultation he has a third heart sound, and his point of maximal impact is displaced laterally. He has 2+ pitting edema of the lower extremities up to the knees. An ECG is obtained and shows premature ventricular complexes and mildly widened QRS complexes. An echocardiogram is also performed and shows global hypokinesis with a left ventricle ejection fraction of 39%. Of the following, what is the most likely cause of his symptoms?
A 14-year-old boy who has been otherwise healthy presents to his doctor complaining of feeling easily winded and light-headed at basketball practice. He has never felt this way before and is frustrated because he is good enough to make varsity this year. He denies smoking, alcohol, or recreational drug use. His mother is very worried because her oldest son and brother had both died suddenly while playing sports despite being otherwise healthy. The transthoracic echocardiogram confirms the suspected diagnosis, which demonstrates a preserved ejection fraction and systolic anterior motion of the mitral valve. The patient is advised that he will need to stay hydrated and avoid intense exercise, and he will likely need an ICD due to his family history. Which of the following physical exam findings is consistent with this patient’s most likely diagnosis?
An 18-year-old boy is brought to the emergency department by his parents because he suddenly collapsed while playing football. His parents mention that he had complained of dizziness while playing before, but never fainted in the middle of a game. On physical examination, the blood pressure is 130/90 mm Hg, the respirations are 15/min, and the pulse is 110/min. The chest is clear, but a systolic ejection murmur is present. The remainder of the examination revealed no significant findings. An electrocardiogram is ordered, along with an echocardiogram. He is diagnosed with hypertrophic cardiomyopathy and the physician lists all the precautions he must follow. Which of the following drugs will be on the list of contraindicated substances?
A 51-year-old man comes to the physician because of progressively worsening dyspnea on exertion and fatigue for the past 2 months. Cardiac examination shows no murmurs or bruits. Coarse crackles are heard at the lung bases bilaterally. An ECG shows an irregularly irregular rhythm with absent p waves. An x-ray of the chest shows globular enlargement of the cardiac shadow with prominent hila and bilateral fluffy infiltrates. Transthoracic echocardiography shows a dilated left ventricle with an ejection fraction of 40%. Which of the following is the most likely cause of this patient's condition?
A 16-year-old boy is brought to the emergency department 20 minutes after collapsing while playing basketball. There is no personal or family history of serious illness. On arrival, there is no palpable pulse and no respiratory effort is seen. He is declared dead. The family agrees to an autopsy. Which of the following is most likely to be found in this patient?
A 73-year-old man with coronary artery disease and hypertension is brought to the emergency department by ambulance 90 minutes after the acute onset of substernal chest pain and dyspnea. He has smoked 2 packs of cigarettes daily for 52 years. Shortly after arriving at the hospital, he loses consciousness and is pulseless. Despite attempts at cardiopulmonary resuscitation, he dies. Examination of the heart at autopsy shows complete occlusion of the left anterior descending artery with a red thrombus overlying a necrotic plaque. Which of the following pathophysiologic mechanisms is most likely responsible for this patient's acute coronary condition?
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app