
Infective endocarditis — MCQs

A 27-year-old man who recently emigrated as a refugee from Somalia presents with fever, weight loss, fatigue, and exertional chest pain. He says his symptoms began 3 weeks ago and that his appetite has decreased and he has lost 3 kg (6.6 lb) in the last 3 weeks. He denies any history of cardiac disease. His past medical history is unremarkable. The patient admits that he has always lived in poor hygienic conditions in overcrowded quarters and in close contact with cats. His vital signs include: blood pressure 120/60 mm Hg, pulse 90/min, and temperature 38.0°C (100.4°F). Physical examination reveals generalized pallor. A cardiac examination reveals an early diastolic murmur loudest at the left third intercostal space. Abdominal examination reveals a tender and mildly enlarged spleen. Prominent axillary lymphadenopathy is noted. Laboratory investigations reveal a WBC count of 14,500/μL with 5% bands and 93% polymorphonuclear cells. An echocardiogram reveals a 5-mm vegetation on the aortic valve with moderate regurgitation. Three sets of blood cultures are taken over 24 hours followed by empiric antibiotic therapy with gentamicin and vancomycin. The blood cultures show no growth after 5 days. Following a week of empiric therapy, the patient continues to deteriorate. Which of the following would most likely confirm the diagnosis in this patient?
A 24-year-old male is brought into the emergency department complaining of chills, headaches, and malaise for several days. He also states that he experiences shortness of breath when climbing two flights of stairs in his home. He admits to occasionally using intravenous drugs during the previous year. On exam, his vital signs are temperature 39.2° C, heart rate 108/min, blood pressure 124/82 mm Hg, respiratory rate 20/min, and oxygen saturation 98% on room air. A holosystolic murmur is heard near the lower left sternal border. An echocardiogram confirms vegetations on the tricuspid valve. What is the most likely causative organism of this patient's condition?
A 37-year-old man presents to the emergency department for a persistent fever. The patient states he has felt unwell for the past week and has felt subjectively febrile. The patient has a past medical history of a suicide attempt and alcohol abuse. He is not currently taking any medications. The patient admits to using heroin and cocaine and drinking 5-8 alcoholic drinks per day. His temperature is 103°F (39.4°C), blood pressure is 92/59 mmHg, pulse is 110/min, respirations are 20/min, and oxygen saturation is 96% on room air. Cardiopulmonary exam is notable for a systolic murmur heard best along the left sternal border. Dermatologic exam reveals scarring in the antecubital fossa. Which of the following is the next best step in management?
A 24-year-old man presents with low-grade fever and shortness of breath for the last 3 weeks. Past medical history is significant for severe mitral regurgitation status post mitral valve replacement five years ago. His temperature is 38.3°C (101.0°F) and respiratory rate is 18/min. Physical examination reveals vertical hemorrhages under his nails, multiple painless erythematous lesions on his palms, and two tender, raised nodules on his fingers. Cardiac auscultation reveals a new-onset 2/6 holosystolic murmur loudest at the apex with the patient in the left lateral decubitus position. A transesophageal echocardiogram reveals vegetations on the prosthetic valve. Blood cultures reveal catalase-positive, gram-positive cocci. Which of the following characteristics is associated with the organism most likely responsible for this patient’s condition?
A 38-year-old female presents to the emergency room with fevers, fatigue, and anorexia for over a month. Past medical history includes mild mitral valve prolapse. She underwent an uncomplicated tooth extraction approximately 6 weeks ago. Her vital signs include a temperature of 100.8 F, pulse of 83, blood pressure of 110/77, and SpO2 of 97% on room air. On exam, you note a grade III/VI holosystolic murmur at the apex radiating to the axilla as well as several red, painful nodules on her fingers. Which of the following is the next best course of action?
Blood cultures are sent to the laboratory. Intravenous antibiotic therapy is started. Transesophageal echocardiography shows a large, oscillating vegetation attached to the tricuspid valve. There are multiple small vegetations attached to tips of the tricuspid valve leaflets. There is moderate tricuspid regurgitation. The left side of the heart and the ejection fraction are normal. Which of the following is the most likely causal organism of this patient's condition?
A 27-year-old man presents to the emergency department with weakness and a fever for the past week. The patient is homeless and has a past medical history of alcohol and IV drug abuse. His temperature is 102°F (38.9°C), blood pressure is 107/68 mmHg, pulse is 120/min, respirations are 17/min, and oxygen saturation is 98% on room air. Physical exam is notable for a tremulous patient with antecubital scars and a murmur over the left lower sternal border. Blood cultures are drawn and the patient is started on vancomycin and ceftriaxone and is admitted to the ICU. The patient's fever and symptoms do not improve despite antibiotic therapy for which the initial identified organism is susceptible. Cultures currently reveal MRSA as one of the infective organisms. Which of the following is the best next step in management?
A 51-year-old man comes to the physician for 2 months of intermittent low-grade fever, malaise, and joint pain. He has a history of recurrent dental abscesses requiring drainage but has otherwise been healthy. His temperature is 38.3°C (100.9°F) and pulse is 112/min. Physical examination shows a new holosystolic murmur in the left midclavicular line that radiates to the axilla. There are linear reddish-brown lesions underneath the nail beds and tender violaceous nodules on the bilateral thenar eminences. Two sets of blood cultures grow Streptococcus mutans. A transthoracic echocardiogram shows moderate regurgitation of the mitral valve. Which of the following mechanisms is most likely directly involved in the pathogenesis of this patient's valvular condition?
A 61-year-old man with a history of stage IIIa lung adenocarcinoma that has been treated with wedge resection and chemotherapy presents to the primary care clinic. He is largely asymptomatic, but he demonstrates a persistent microcytic anemia despite iron supplementation. Colonoscopy performed 3 years earlier was unremarkable. His past medical history is significant for diabetes mellitus type II, hypertension, acute lymphoblastic leukemia as a child, and hypercholesterolemia. He currently smokes 1 pack of cigarettes per day, drinks a glass of pinot grigio per day, and currently denies any illicit drug use. His vital signs include: temperature, 36.7°C (98.0°F); blood pressure, 126/74 mm Hg; heart rate, 87/min; and respiratory rate, 17/min. On physical examination, his pulses are bounding, complexion is pale, but breath sounds remain clear. Oxygen saturation was initially 91% on room air, with a new oxygen requirement of 2 L by nasal cannula. Which of the following lab values would suggest anemia of chronic disease as the underlying etiology?
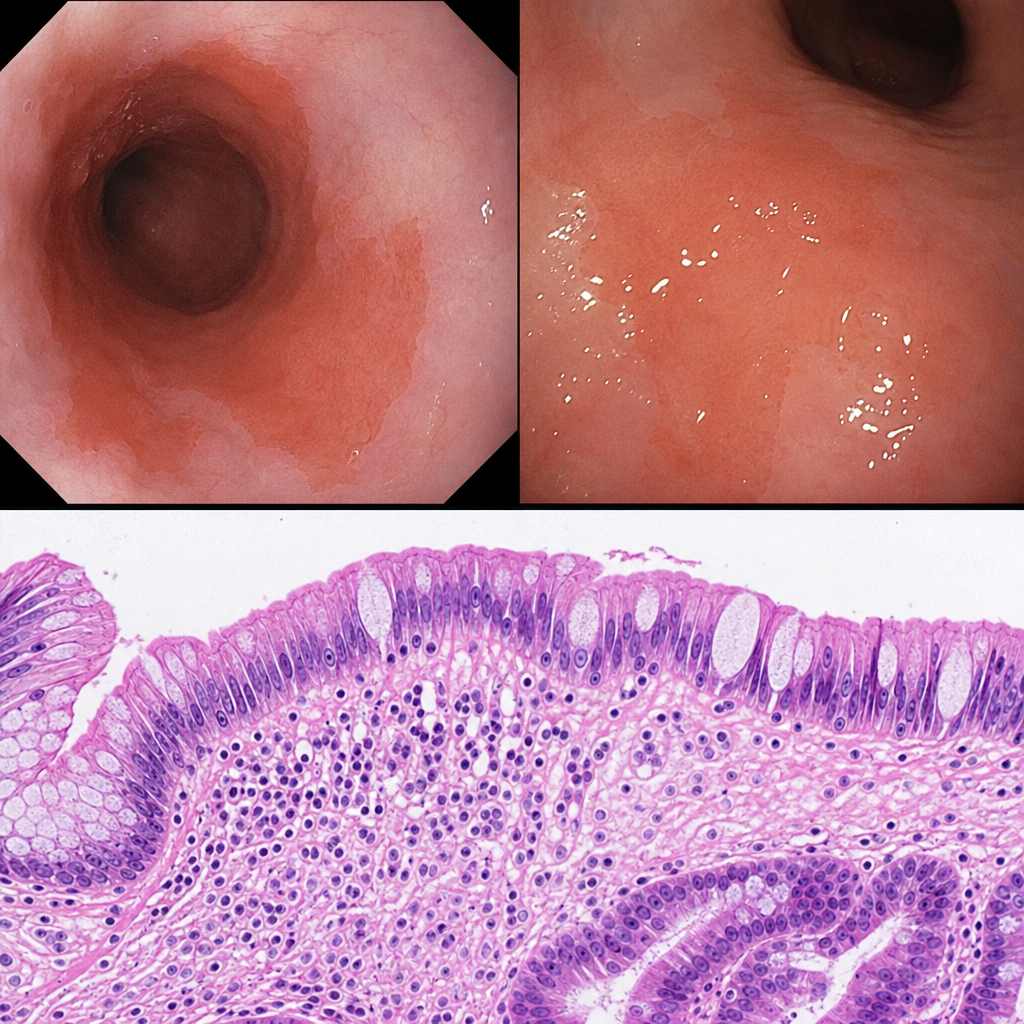
A 67-year-old man with a long-standing history of gastroesophageal reflux disease undergoes upper endoscopy. A biopsy from 2 cm above the gastroesophageal junction is obtained from an area of salmon-colored mucosa. Histological examination shows replacement of the normal squamous epithelium by columnar epithelium containing goblet cells interspersed among columnar absorptive cells, with intact basement membrane and no nuclear stratification, pleomorphism, or loss of polarity. Which of the following statements most accurately characterizes the biological behavior and reversibility of this histological change?
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app